OK. Again, we know it wasn't a trauma ABG! But, it's a great ABG for doing some more practice, and it has real comments from the examiners attached.
So, how did you go in that very generous six minutes we gave you?
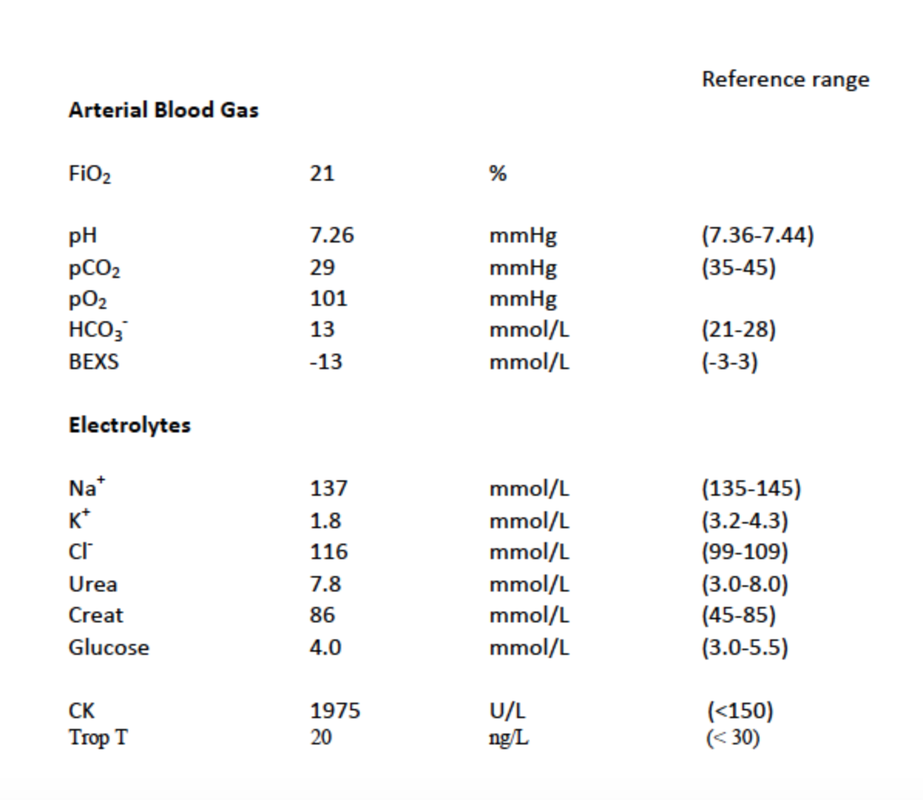
To pass the exam standard, you should be able to write down:
ACID BASE BALANCE
Mild acidaemia
Metabolic acidosis
Expected CO2 of 27.5 therefore appropriate respiratory compensation
AG of 8 therefore diagnose NAGMA
OXYGENATION
Aa gradient of 12 (very close to expected, no serious V/Q mismatch).
ELECTROYLTES
Critical hypokalaemia - likely the cause of the weakness (and a risk for VF!)
Mild elevation of CK with preservation of renal function
Mild chloride elevation (renal retention of chloride for NAGMA)
INTERPRETATION
Therefore should consider as underlying diagnoses:
- renal pathology (RTA)
- acetazolamide toxicity
- other bicarbonate loss (?laxative abuse syndrome).
That's it! Take it from us, you need to be able to get through that in six minutes. For the record, the examiner's comments from the 2013.1 examination report are below for your information. Have a read - they are an interesting insight into the examiner's approach to marking questions. The pass rate of 46% is also an interesting comment on candidate's abilities to do an ABG question. In the new exam you will probably end up with a more directed question (similar to the ones we are asking) but you need to able to assess and deconstruct an ABG on its own merits.
To pass the exam standard, you should be able to write down:
ACID BASE BALANCE
Mild acidaemia
Metabolic acidosis
Expected CO2 of 27.5 therefore appropriate respiratory compensation
AG of 8 therefore diagnose NAGMA
OXYGENATION
Aa gradient of 12 (very close to expected, no serious V/Q mismatch).
ELECTROYLTES
Critical hypokalaemia - likely the cause of the weakness (and a risk for VF!)
Mild elevation of CK with preservation of renal function
Mild chloride elevation (renal retention of chloride for NAGMA)
INTERPRETATION
Therefore should consider as underlying diagnoses:
- renal pathology (RTA)
- acetazolamide toxicity
- other bicarbonate loss (?laxative abuse syndrome).
That's it! Take it from us, you need to be able to get through that in six minutes. For the record, the examiner's comments from the 2013.1 examination report are below for your information. Have a read - they are an interesting insight into the examiner's approach to marking questions. The pass rate of 46% is also an interesting comment on candidate's abilities to do an ABG question. In the new exam you will probably end up with a more directed question (similar to the ones we are asking) but you need to able to assess and deconstruct an ABG on its own merits.
FACEM VAQ Exam 2013.1 – Question 3
- The overall pass rate for this question was 62/134 (46.3%)
- In the description
- Profound hypokalaemia
- Non-AG metabolic acidosis with respiratory compensation
- Increased CK
- Normal renal function
- In the interpretation
- Hypokalaemia most likely cause of weakness
- CK rise not excessive, unlikely cause of weakness
- Causes:
- RTA must be mentioned
- PLUS at least one other NAGMA with rationalisation for inclusion/exclusion
- Expected features of better answers
- Increased Chloride noted
- Causes of CK in the range of this result (mild)
- Commentary regarding pO2 and A/a gradient
- Interpretation of NAGMA cause focused on stem and not overly inclusive without qualification
- Features of unsuccessful answer
- Candidates scored poorly largely due to poor interpretation. Comparing a parameter to a normal range and then stating “high”, “low” or “normal” is not interpretation and scores very little as description. Candidates should always try to interpret the results in light of the clinical situation described.
- Several candidates did calculations for expected CO2 or A-a grad, but then made no or little comment on the result. A calculation is only useful if the result is correctly interpreted. Interpretation requires specific comment from the candidate. Marks are scored for clinical correlation of the result, not the actual calculation.
- Many candidates failed to interpret the results in light of the stem of the question. In particular, many patients missed the association between the patient’s very low potassium and his weakness.
- Many candidates failed to adapt their answers to the question and interpret “on the run”. An example of this is the AG calculation. Many recognised the metabolic acidosis but didn’t quantify the type of acidosis until much later in their answer as they did not perform the AG calculation until later. A better approach would be to perform the appropriate calculation at the appropriate time. This demonstrates a better understanding of concepts.
- Some candidates failed to appreciate that all calculations have a margin of error (often +/- 1-2). In many cases, this led to the erroneous assumption that respiratory compensation was either not complete or over-exaggerated. This caused candidates to erroneously assume there was also a primary respiratory problem.
- Several candidates performed delta gap calculations incorrectly. Again this led to erroneous interpretation. (Most experts would suggest that delta gap should only be performed in setting of HAGMA).
- The CK was poorly interpreted by many. Whilst elevated, a CK of 1975 is not likely to cause significant Rhabdomyolysis.
- Candidates who scored poorly often wrote contradictory information in their lists eg. rhabdomyolysis and renal failure as a cause of high CK, after saying that renal function was normal in their description.