MODULE 24.
Well - here we are. The exam is approaching very rapidly, and you are probably getting very sick of study....So, use this module to catch up and prepare yourself. If you've nothing better to do, the MCQ generator is still available to spot test your knowledge, and below is a final set of questions that Peter has set to make you think about some important topics.
Watch: some final words from Peter.
| some_final_words_from_luke.pdf |
solve: peter's pot pouri of revision.
I have called this a POT POURI of revision. these are topics that you need to know so lets make sure there are no gaps.
QUESTION 1
A 78 yo woman is brought to the emergency department with increased confusion. According to the nursing home she has been eating and drinking normally until 2 days ago.
Her vitals are essentially normal.
A Stat set of bloods comes back with the following results:
Na 122 mmol/L
K 4.6 mmol/L
Cl 109 mmol/L
Urea 3.4 mol/L
Cr 108 mol/L
Question 1. (3 marks)
Describe these results.
Question 2. (3 marks)
What 3 other tests would you need to do to determine the cause of the abnormality.
Question 3. (5 marks)
How would you correct this abnormality?
Her vitals are essentially normal.
A Stat set of bloods comes back with the following results:
Na 122 mmol/L
K 4.6 mmol/L
Cl 109 mmol/L
Urea 3.4 mol/L
Cr 108 mol/L
Question 1. (3 marks)
Describe these results.
Question 2. (3 marks)
What 3 other tests would you need to do to determine the cause of the abnormality.
Question 3. (5 marks)
How would you correct this abnormality?
ANSWER
1 This patient has a low Na and a low Cl; diagnosis hyponatraemia
2 The other tests needed to diagnose the cause of hyponatraemia are:
-Osmolality; Urine and Serum
-Urine Na Concentration
Urine osmolality helps with determining if the cause is psychogenic polydipsia or ADH secretion.
In a normal functioning kidney the urine osmolality is < 100mOsmol/kg
Urinary Na helps to differentiate between hypovolaemia and SIADH. Remember SIADH is a salt wasting syndrome, so the urinary salt is >20-40 mmol/L.
Watch the following video again for the diagnosis of hyponatraemia:
2 The other tests needed to diagnose the cause of hyponatraemia are:
-Osmolality; Urine and Serum
-Urine Na Concentration
Urine osmolality helps with determining if the cause is psychogenic polydipsia or ADH secretion.
In a normal functioning kidney the urine osmolality is < 100mOsmol/kg
Urinary Na helps to differentiate between hypovolaemia and SIADH. Remember SIADH is a salt wasting syndrome, so the urinary salt is >20-40 mmol/L.
Watch the following video again for the diagnosis of hyponatraemia:
3. Treatment of this condition must be controlled as there are potential sequelae if not done properly, we can cause the patient harm.
In symptomatic patients with acute hyponatremia (ie, with a known duration of <24-48 hours), urgent correction by 4-6 mmol/L to prevent brain herniation and neurological damage from cerebral ischemia. This can be done by:
In symptomatic patients with acute hyponatremia (ie, with a known duration of <24-48 hours), urgent correction by 4-6 mmol/L to prevent brain herniation and neurological damage from cerebral ischemia. This can be done by:
- Severe symptoms: 100 mL of 3% NaCl infused intravenously over 10 minutes × 3 as needed
- Mild to moderate symptoms, in patients at low risk for herniation: 3% NaCl infused at 0.5–2 mL/kg/h
- Minimum correction of serum sodium by 4-8 mmol/L per day, with a lower goal of 4-6 mmol/L per day if the risk of ODS is high
- For patients at high risk of ODS: maximum correction of 8 mmol/L in any 24-hour period
- For patients at normal risk of ODS: maximum correction of 10-12 mmol/L in any 24-hour period; 18 mmol/L in any 48-hour period
QUESTION 2
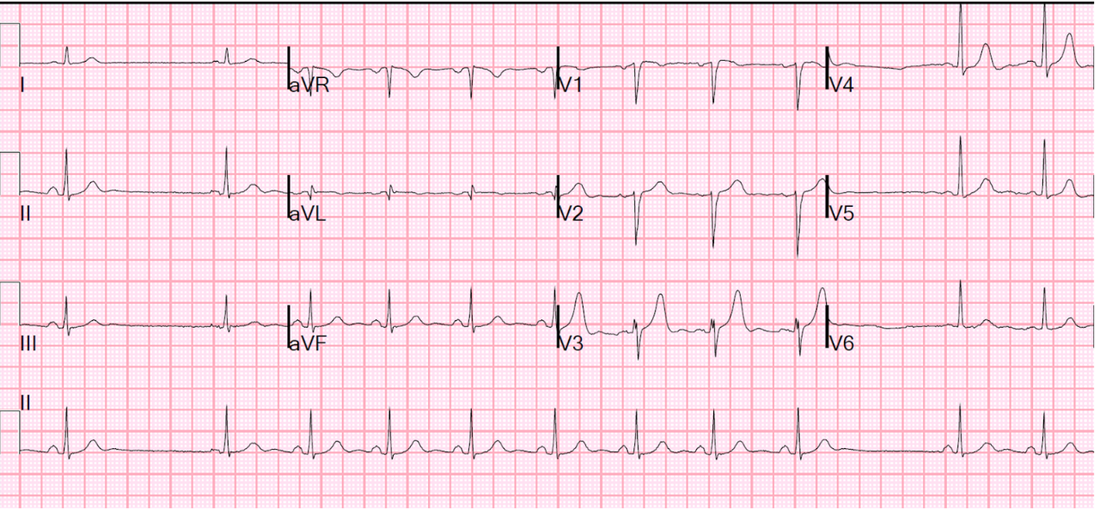
A 24 yo male presents with palpitations. He has no other symptoms, has had no previous medical history and is on no medications. His is afebrile. His ECG is shown below:
Question 1.
Describe the ECG.
Question 2.
What is the diagnosis?
Question 3.
How do you treat this patient?
Question 1.
Describe the ECG.
Question 2.
What is the diagnosis?
Question 3.
How do you treat this patient?
answer
This gentleman has a sinatorial exit block.
Do you know the difference between these blocks:
1. Sinus pause: At least 2 seconds of pause
2. Sinus arrest: No P-waves. asystole is a possible outcome of sinus arrest.
The pause length may not be a multiple of the basic sinus rate.
3. Sinoatrial nodal exit block: The impulse from the pacemaker cells is not transmitted so there are no P waves
This may be a multiple of the basic sinus rate.
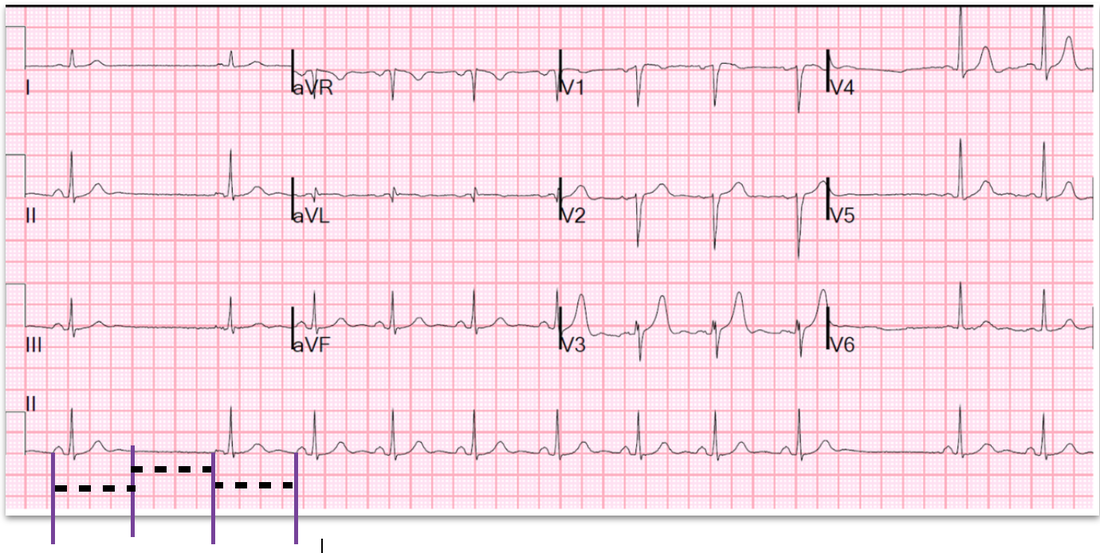
If you look at the ECG below, the missed P wave is a multiple of the basic sinus rate.
Do you know the difference between these blocks:
1. Sinus pause: At least 2 seconds of pause
2. Sinus arrest: No P-waves. asystole is a possible outcome of sinus arrest.
The pause length may not be a multiple of the basic sinus rate.
3. Sinoatrial nodal exit block: The impulse from the pacemaker cells is not transmitted so there are no P waves
This may be a multiple of the basic sinus rate.
If you look at the ECG below, the missed P wave is a multiple of the basic sinus rate.
How to treat this patient?
There is no real treatment necessary. There may be some reversible causes including those related to drugs such as digoxin, amiodarone, beta blockers. Myocardial infarction can also cause it. Sick sinus syndrome may also be involved.
Usually if the patient only has palpitations and no syncope, no treatment is necessary.
There is no real treatment necessary. There may be some reversible causes including those related to drugs such as digoxin, amiodarone, beta blockers. Myocardial infarction can also cause it. Sick sinus syndrome may also be involved.
Usually if the patient only has palpitations and no syncope, no treatment is necessary.
question 3
,A 75 yo woman is brought into the emergency department following being found outside on the ground all night. Her conscious state is depressed and she has a temperature of 29C, with fixed dilated pupils.
Question 1.
How do you define hypothermia?
Question 2.
Name 3 different systems it affects and how it affects them.
Question 3.
On presentation the patient was in atrial fibrillation. In your resuscitation bay, the rhythm changes to ventricular fibrillation(VF). She has 3 shocks at 200J and is still in VF. Give 5 specifics about management of this patient in cardiac arrest.
Question 1.
How do you define hypothermia?
Question 2.
Name 3 different systems it affects and how it affects them.
Question 3.
On presentation the patient was in atrial fibrillation. In your resuscitation bay, the rhythm changes to ventricular fibrillation(VF). She has 3 shocks at 200J and is still in VF. Give 5 specifics about management of this patient in cardiac arrest.
ANswer
Hypothermia defined as < 35C
Mild 32-35, Moderate 28-32, Severe <28
It affects most systems- Think of it as slowing everything down:
CVS: Bradycardia, hypotension
CNS: Neuroprotective, FIXED DILATED PUPILS occur at temp < 30C
RESP: decreased CO2, Decreased PaO2
RENAL: Decreased GFR. Cold Induced diuresis.
Cardiac arrest management in these patients can be quite tricky and lengthy.
How do you rewarm? You need to look this up and know it, as well as how quickly patients warm up.
I think of it as peripheral or central warming.
IV fluid is 42C. Body cavity lavage usually uses fluid at 40C
Mild 32-35, Moderate 28-32, Severe <28
It affects most systems- Think of it as slowing everything down:
CVS: Bradycardia, hypotension
CNS: Neuroprotective, FIXED DILATED PUPILS occur at temp < 30C
RESP: decreased CO2, Decreased PaO2
RENAL: Decreased GFR. Cold Induced diuresis.
Cardiac arrest management in these patients can be quite tricky and lengthy.
- If their temperature is < 30C, they get one lot of 3 shocks if in VF
- Any other rhythm, you would leave alone.
- No more shocks until temperature is >30C.
- Also no adrenaline until temp >30.
- CPR may have to be done for several hours until rewarmed.
How do you rewarm? You need to look this up and know it, as well as how quickly patients warm up.
I think of it as peripheral or central warming.
- Peripheral warming is about rewarming blankets etc that raise your temperature at a rate of 2 degrees/hour.
- Central warming is about humidified gas, warm IV fluids(don't change much) and body cavity lavage ie., peritoneal lavage(raises temperature by 3degrees per hour), gastric, bladder or thoracic cage.
IV fluid is 42C. Body cavity lavage usually uses fluid at 40C
Question 4
A 4 yo boy is brought to the emergency department by ambulance. He was in the back seat of a car, that was involved in a high speed collision, with the driver, now intubated, with significant head injuries.
The child is alert and has some left sided neck pain.
Question 1.
How do approach clearing the cervical spine in this child?
The child is alert and has some left sided neck pain.
Question 1.
How do approach clearing the cervical spine in this child?
ANSWER
Clearing cervical spines in children is a common sense approach that can use the NEXUS criteria, less of the CT and more plain Xray for imaging.
The literature is not quite clear on this. If you have an approach, use it. If you don't adopt one and use it.
My approach based on Emerg Med J 2004 March 21(2)189-193 is as follows:
The literature is not quite clear on this. If you have an approach, use it. If you don't adopt one and use it.
My approach based on Emerg Med J 2004 March 21(2)189-193 is as follows:
- If the child is alert and asymptomatic with a normal examination=> Clear clinically
- If the child is alert with minor neck pain and no neurology treat with simple analgesia and review. If assymptomatic=>clear
- If the child has cervical spine symptoms and signs=> perform plain Xray, if suspicious or poorly defined areas, consider CT
- If the child has an impaired conscious state, consider plain Xray , complimented by MRI
QUESTION 5
A 35yo patient presents with multiple complaints including:
This is a previously well patient with no significant history. There were some mild flu-like symptoms this morning on waking. During the day the patient developed severe cramping abdominal pain that was burning in nature. It radiated to the epigastrium and retrosternally.
The patient then developed burning pain between the scapulae as well as lumbar back pain, followed by numbness and weakness of both legs, the numbness extending to the abdomen, to T10. The patient was unable to stand and pass urine.
The patient was alert and in no distress. Examination revealed normal vitals, with dual heart sounds and no extra sounds, a clear chest and a soft abdomen with a mild epigastric discomfort.
Spinal examination demonstrated some tenderness over L5. Neurological examination demonstrated sensory loss, as well as loss of pain sensation from T10 distally.
Lower limb examination demonstrated normal tone bilaterally. Power was 0/5 in the whole right leg. The left leg had 3/5 power at the ankle and knee and 1/5 at the hip. Both plantars were down-going and no reflexes were present.
What's your diagnosis from the clinical picture?
Pick an answer from below: Don't get too stressed if you don't know this (it's very detailed) but you do need to know the causes of the patient who presents with BACK PAIN and need to know about (a) and (d) - (f) in the list below.
(a) Brown-Sequard Syndrome
(b) Haematomyelia
(c) Neurosyphilis
(d) Transverse Myelitis
(e) Spinal Cord Infarction
(f) Demyelinating Disease
- lower abdominal pain
- retrosternal chest pain
- lumber back pain and
- numbness and weakness in both legs
This is a previously well patient with no significant history. There were some mild flu-like symptoms this morning on waking. During the day the patient developed severe cramping abdominal pain that was burning in nature. It radiated to the epigastrium and retrosternally.
The patient then developed burning pain between the scapulae as well as lumbar back pain, followed by numbness and weakness of both legs, the numbness extending to the abdomen, to T10. The patient was unable to stand and pass urine.
The patient was alert and in no distress. Examination revealed normal vitals, with dual heart sounds and no extra sounds, a clear chest and a soft abdomen with a mild epigastric discomfort.
Spinal examination demonstrated some tenderness over L5. Neurological examination demonstrated sensory loss, as well as loss of pain sensation from T10 distally.
Lower limb examination demonstrated normal tone bilaterally. Power was 0/5 in the whole right leg. The left leg had 3/5 power at the ankle and knee and 1/5 at the hip. Both plantars were down-going and no reflexes were present.
What's your diagnosis from the clinical picture?
Pick an answer from below: Don't get too stressed if you don't know this (it's very detailed) but you do need to know the causes of the patient who presents with BACK PAIN and need to know about (a) and (d) - (f) in the list below.
(a) Brown-Sequard Syndrome
(b) Haematomyelia
(c) Neurosyphilis
(d) Transverse Myelitis
(e) Spinal Cord Infarction
(f) Demyelinating Disease
ANSWER
The answer is (e).
The main reason for this:
The process was rapid onset- acute, which is in line with a vascular event.
Brown-Sequard- has ipsilateral paralysis and loss of proprioception and contralateral loss of pain and temperature
Transverse Myelitis- When this occurs in the thoracic region, the patient has upper motor neurone signs in the lower limbs and spastic diplegia
Spinal Cord Infarction- This behaves like a spinal shock, with flaccid paralysis, loss of tone and areflexia.
The main reason for this:
The process was rapid onset- acute, which is in line with a vascular event.
Brown-Sequard- has ipsilateral paralysis and loss of proprioception and contralateral loss of pain and temperature
Transverse Myelitis- When this occurs in the thoracic region, the patient has upper motor neurone signs in the lower limbs and spastic diplegia
Spinal Cord Infarction- This behaves like a spinal shock, with flaccid paralysis, loss of tone and areflexia.
write: the exam!
If there are any final questions/anxieties please contact us.
Good luck!
Peter and Luke
Good luck!
Peter and Luke