MODULE FOUR short answer questions.
saq 1.
A 50 year old female presents to your department after a heroin overdose. Her vital signs are:
HR 76 /min
BP 90/62 mmHg
RR 3 /min
O2 sats 2L 96% 2L via prongs
T 37.2 oC
An arterial blood gas is shown below.
FiO2 28%
pH 7.20
pO2 87 mmHg
PCO2 105 mmHg
HCO3- 30 mmol/L
BE +8
Question 1. What are the major acid base disturbances? (3 marks)
Must include:
- mild-moderate acidaemia
- respiratory acidosis
- (compensatory) metabolic alkalosis
Question 2. What is the primary acid-base disturbance? (1 mark)
Respiratory acidosis.
Question 3. What HCO3- levels would you expect as acute and chronic compensation for the primary disturbance? (2 marks)
Acutely 30mmol/L
Bicarbonate rises by 1 for each 10mmHg of CO2 over 40mmHg
Chronically 50mmol/L
Bicarbonate rises by 4 for each 10mmHg of CO2 over 40mmHg
Question 4. Is there a V/Q mismatch, or is the primary problem hypoventilation? Why? (4 marks)
There is no V/Q mismatch.
The Aa gradient is calculated as:
225mmHg - 87 - 105 x 1.25
= 225 - 87 - 131
= 225 - 228
= 7mmHg.
The expected Aa gradient for a patient this age is 50/4 + 4 = 16.5.
Therefore the Aa gradient is normal, and no V/Q mismatch exists.
***NOTE, one of our candidates asked why we used 225mmHg for 28% oxygen. This is a great question, and we have left our original answer and the update here for everyone's information. Thanks Ignatius!***
For the examination, where no calculators are allowed (yes, seriously) you need to have something that works well for calculating alveolar oxygen pressure.
If you remember at sea level that the first number in the alveolar gas equation is 150 (on 21% oxygen, you can calculate through the Aa gradient for different FiO2s).
Out of (call it intellectual laziness if you want!) Luke used to approximate Oxygen values as follows:
- 21% = 150 mmHg
- 28% (1.5 x 21%) = 225mmHg
- 40% (2 x 21%) = 300 mmHg
- 60% (3 x 21%) = 450 mmHg.
Of course, a better approximation for 28% oxygen is 1.3 x 21%, i.e. 200mmHg. Rarely will it make an examination difference (and never in clinical practice!!!!) but it's worth using the most accurate approximation.
HR 76 /min
BP 90/62 mmHg
RR 3 /min
O2 sats 2L 96% 2L via prongs
T 37.2 oC
An arterial blood gas is shown below.
FiO2 28%
pH 7.20
pO2 87 mmHg
PCO2 105 mmHg
HCO3- 30 mmol/L
BE +8
Question 1. What are the major acid base disturbances? (3 marks)
Must include:
- mild-moderate acidaemia
- respiratory acidosis
- (compensatory) metabolic alkalosis
Question 2. What is the primary acid-base disturbance? (1 mark)
Respiratory acidosis.
Question 3. What HCO3- levels would you expect as acute and chronic compensation for the primary disturbance? (2 marks)
Acutely 30mmol/L
Bicarbonate rises by 1 for each 10mmHg of CO2 over 40mmHg
Chronically 50mmol/L
Bicarbonate rises by 4 for each 10mmHg of CO2 over 40mmHg
Question 4. Is there a V/Q mismatch, or is the primary problem hypoventilation? Why? (4 marks)
There is no V/Q mismatch.
The Aa gradient is calculated as:
225mmHg - 87 - 105 x 1.25
= 225 - 87 - 131
= 225 - 228
= 7mmHg.
The expected Aa gradient for a patient this age is 50/4 + 4 = 16.5.
Therefore the Aa gradient is normal, and no V/Q mismatch exists.
***NOTE, one of our candidates asked why we used 225mmHg for 28% oxygen. This is a great question, and we have left our original answer and the update here for everyone's information. Thanks Ignatius!***
For the examination, where no calculators are allowed (yes, seriously) you need to have something that works well for calculating alveolar oxygen pressure.
If you remember at sea level that the first number in the alveolar gas equation is 150 (on 21% oxygen, you can calculate through the Aa gradient for different FiO2s).
Out of (call it intellectual laziness if you want!) Luke used to approximate Oxygen values as follows:
- 21% = 150 mmHg
- 28% (1.5 x 21%) = 225mmHg
- 40% (2 x 21%) = 300 mmHg
- 60% (3 x 21%) = 450 mmHg.
Of course, a better approximation for 28% oxygen is 1.3 x 21%, i.e. 200mmHg. Rarely will it make an examination difference (and never in clinical practice!!!!) but it's worth using the most accurate approximation.
saq 2.
A 21 year old man with a history of insulin dependent diabetes presents to the emergency department with an altered level of consciousness.
His vital signs are:
HR 115 /min
BP 105/73 mmHg
RR 30 /min
O2 sats 2L 99% RA
T 37.3 oC
An arterial blood gas is shown below.
FiO2 21%
pH 7.15
pO2 114 mmHg
PCO2 20 mmHg
HCO3- 8 mmol/L
BE -16
Na+ 140 mmol/L
K+ 6.0 mmol/L
Cl- 110 mmol/L
Question 1. What are the major acid base disturbances? (3 marks)
Moderate acidaemia
Metabolic acidosis
Compensatory respiratory alkalosis
Question 2. What is the primary disturbance? (1 mark)
Metabolic acidosis
Question 3. What CO2 level would you expect as compensation for the primary acid-base disturbance? (1 mark)
Expect CO2 = 20mmHg
Question 4. What is the anion gap? (1 mark)
AG = 22 (raised)
Question 5. Give 4 acids that are causes of a raised anion gap? (4 marks)
Lactic acid
Ketoacids
Uraemia
Salicylates
His vital signs are:
HR 115 /min
BP 105/73 mmHg
RR 30 /min
O2 sats 2L 99% RA
T 37.3 oC
An arterial blood gas is shown below.
FiO2 21%
pH 7.15
pO2 114 mmHg
PCO2 20 mmHg
HCO3- 8 mmol/L
BE -16
Na+ 140 mmol/L
K+ 6.0 mmol/L
Cl- 110 mmol/L
Question 1. What are the major acid base disturbances? (3 marks)
Moderate acidaemia
Metabolic acidosis
Compensatory respiratory alkalosis
Question 2. What is the primary disturbance? (1 mark)
Metabolic acidosis
Question 3. What CO2 level would you expect as compensation for the primary acid-base disturbance? (1 mark)
Expect CO2 = 20mmHg
Question 4. What is the anion gap? (1 mark)
AG = 22 (raised)
Question 5. Give 4 acids that are causes of a raised anion gap? (4 marks)
Lactic acid
Ketoacids
Uraemia
Salicylates
saq 3.
A 21 year old girl presents complaining of severe chest pain and shaking in the hands. She is acutely distressed, and states that the pain came on after an argument with her boyfriend.
Her vital signs are:
HR 128 /min
BP 109/79 mmHg
RR 38 /min
O2 sats 2L 99% RA
T 37.0 oC
An arterial blood gas is taken by the intern.
FiO2 21%
pH 7.55
PO2 115 mmHg
PCO2 22 mmHg
HCO3- 20 mmol/L
BE +4
Question 1. What are the major acid base disturbances? (3 marks)
Must include:
- mild-moderate alkalaemia
- respiratory alkalosis
- metabolic acidosis
Question 2. What is the primary acid-base disturbance? (1 mark)
Respiratory alkalosis.
Question 3. What HCO3- levels would you expect as acute and chronic compensation for the primary disturbance? (2 marks)
Acutely 20mmol/L
Bicarbonate falls by 2 for each 10mmHg of CO2 below 40mmHg
Chronically 14mmol/L
Bicarbonate falls by 5 for each 10mmHg of CO2 below 40mmHg
Question 4. What is the Aa gradient? (2 marks)
The Aa gradient is calculated as:
150mmHg - 115 - 22 x 1.25
=150 - 115 - 27.5
= 150 - 142.5
= 7.5mmHg.
The expected Aa gradient for a patient this age is 21/4 + 4 = 9.25.
Therefore the Aa gradient is normal, and no V/Q mismatch exists.
Question 5. What is the likely diagnosis? (2 marks)
Must include:
Acute anxiety disorder
Her vital signs are:
HR 128 /min
BP 109/79 mmHg
RR 38 /min
O2 sats 2L 99% RA
T 37.0 oC
An arterial blood gas is taken by the intern.
FiO2 21%
pH 7.55
PO2 115 mmHg
PCO2 22 mmHg
HCO3- 20 mmol/L
BE +4
Question 1. What are the major acid base disturbances? (3 marks)
Must include:
- mild-moderate alkalaemia
- respiratory alkalosis
- metabolic acidosis
Question 2. What is the primary acid-base disturbance? (1 mark)
Respiratory alkalosis.
Question 3. What HCO3- levels would you expect as acute and chronic compensation for the primary disturbance? (2 marks)
Acutely 20mmol/L
Bicarbonate falls by 2 for each 10mmHg of CO2 below 40mmHg
Chronically 14mmol/L
Bicarbonate falls by 5 for each 10mmHg of CO2 below 40mmHg
Question 4. What is the Aa gradient? (2 marks)
The Aa gradient is calculated as:
150mmHg - 115 - 22 x 1.25
=150 - 115 - 27.5
= 150 - 142.5
= 7.5mmHg.
The expected Aa gradient for a patient this age is 21/4 + 4 = 9.25.
Therefore the Aa gradient is normal, and no V/Q mismatch exists.
Question 5. What is the likely diagnosis? (2 marks)
Must include:
Acute anxiety disorder
saq 4.
A 61 year old female presents to your department with a distended abdomen and copious vomiting which has worsened for the past 12 hours. She is complaining of extreme thirst, and has had three vomits since she arrived in your department 45 minutes previously. She has a history of bowel obstructions due to adhesions from previous surgery.
HR 116 /min
BP 115/74 mmHg
RR 8 /min
O2 sats 2L 99% RA
T 37.3 oC
An arterial blood gas is shown below.
FiO2 21%
pH 7.55
pO2 94 mmHg
PCO2 45 mmHg
HCO3- 32 mmol/L
BE +8
Question 1. What are the major acid base disturbances? Indicate the primary derangement. (4 marks)
Must include: (1 mark each)
- moderate alkalaemia
- metabolic alkalosis(primary, for an extra mark)
- borderline respiratory acidosis
Question 2. What CO2 levels would you expect as compensation for the primary disturbance? (2 marks)
Expected CO2 in a metabolic alkalosis = 20 + 0.8x[HCO3-]
Therefore expect 20 + 0.8x32 ~45mmHg
Question 3. Why does the patient have their acid base disturbance?(1 mark)
Must include:
Significant HCl loss due to excessive vomiting
Question 4. What further investigations will you order?
Must include:
Abdominal imaging: either CT or XRAY (at a minimum)
UEC - check hypochloraemia and renal failure
Plus any from (0.5 marks each up to 1 mark):
- Lactate level
- Liver function
- Lipase
- Urinalysis
- FBC
HR 116 /min
BP 115/74 mmHg
RR 8 /min
O2 sats 2L 99% RA
T 37.3 oC
An arterial blood gas is shown below.
FiO2 21%
pH 7.55
pO2 94 mmHg
PCO2 45 mmHg
HCO3- 32 mmol/L
BE +8
Question 1. What are the major acid base disturbances? Indicate the primary derangement. (4 marks)
Must include: (1 mark each)
- moderate alkalaemia
- metabolic alkalosis(primary, for an extra mark)
- borderline respiratory acidosis
Question 2. What CO2 levels would you expect as compensation for the primary disturbance? (2 marks)
Expected CO2 in a metabolic alkalosis = 20 + 0.8x[HCO3-]
Therefore expect 20 + 0.8x32 ~45mmHg
Question 3. Why does the patient have their acid base disturbance?(1 mark)
Must include:
Significant HCl loss due to excessive vomiting
Question 4. What further investigations will you order?
Must include:
Abdominal imaging: either CT or XRAY (at a minimum)
UEC - check hypochloraemia and renal failure
Plus any from (0.5 marks each up to 1 mark):
- Lactate level
- Liver function
- Lipase
- Urinalysis
- FBC
saq 5.
A 52 year old smoker on home oxygen for COPD present feeling generally unwell. On further questioning he describes a fever and a cough for several days.
His vital signs are:
HR 123 /min
BP 98/71 mmHg
RR 42 /min
O2 sats 2L 89% 6L
T 39.6 oC
An arterial blood gas is taken.
FiO2 40%
pH 7.12
pO2 60 mmHg
PCO2 75 mmHg
HCO3- 16 mmol/L
BE -1
Na+ 145 mmol/L
Cl- 101 mmol/L
Lactate 5.4 mmol/L
Question 1. What are the major acid base disturbances? Indicate the primary derangement. (4 marks)
Must include: (1 mark each)
- severe acidaemia
- metabolic acidosis
- respiratory acidosis
Question 2. Which of these is the primary disturbance? (1 mark)
These are 2 independent processes representative of independent primary pathologies (infective COAD and sepsis).
Question 3. What is the anion gap? (1 mark)
AG = 145 - (101+14) = 30
Question 4. Is there a metabolic alkalosis present? Justify your answer.
Must include: (Score 2 marks for delta ratio calculation, and 2 marks for an explanation).
DELTA ratio = (change in anion gap)/(change in HCO3-)
= (30-12)/(24-16)
= 18/8
>2.0.
The high delta ratio implies a co-existing, or pre-existing metabolic alkalosis underneath the acidosis, in this case most likely because of chronic CO2 retention with consquent chronic metabolic alkalosis as compensation.
Would also accept as an explanation the idea that the fall in bicarbonate is discrepant with the base excess, implying a resting bicarbonate of >24.
However, without a delta ratio, or reference to base excess, candidates score NO MARKS.
His vital signs are:
HR 123 /min
BP 98/71 mmHg
RR 42 /min
O2 sats 2L 89% 6L
T 39.6 oC
An arterial blood gas is taken.
FiO2 40%
pH 7.12
pO2 60 mmHg
PCO2 75 mmHg
HCO3- 16 mmol/L
BE -1
Na+ 145 mmol/L
Cl- 101 mmol/L
Lactate 5.4 mmol/L
Question 1. What are the major acid base disturbances? Indicate the primary derangement. (4 marks)
Must include: (1 mark each)
- severe acidaemia
- metabolic acidosis
- respiratory acidosis
Question 2. Which of these is the primary disturbance? (1 mark)
These are 2 independent processes representative of independent primary pathologies (infective COAD and sepsis).
Question 3. What is the anion gap? (1 mark)
AG = 145 - (101+14) = 30
Question 4. Is there a metabolic alkalosis present? Justify your answer.
Must include: (Score 2 marks for delta ratio calculation, and 2 marks for an explanation).
DELTA ratio = (change in anion gap)/(change in HCO3-)
= (30-12)/(24-16)
= 18/8
>2.0.
The high delta ratio implies a co-existing, or pre-existing metabolic alkalosis underneath the acidosis, in this case most likely because of chronic CO2 retention with consquent chronic metabolic alkalosis as compensation.
Would also accept as an explanation the idea that the fall in bicarbonate is discrepant with the base excess, implying a resting bicarbonate of >24.
However, without a delta ratio, or reference to base excess, candidates score NO MARKS.
SAQ 6.
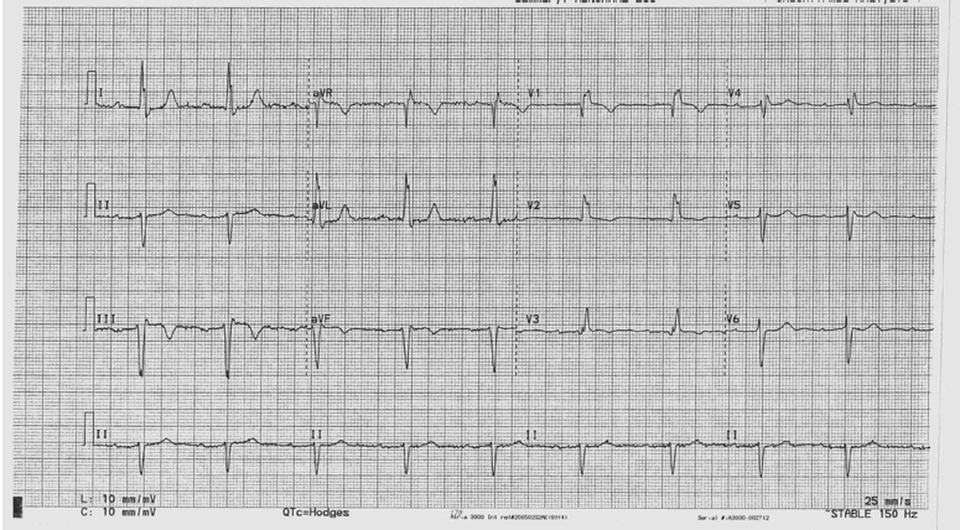
A 79 year old man presents with "palpitations". He has never had them before, and says they began yesterday. He has developed a productive cough and intermittent fevers over the last three days.
His presentation ECG is shown below. Although not specified please assume standard calibration. (25mm/s & 1mV to 10mm)
His presentation ECG is shown below. Although not specified please assume standard calibration. (25mm/s & 1mV to 10mm)
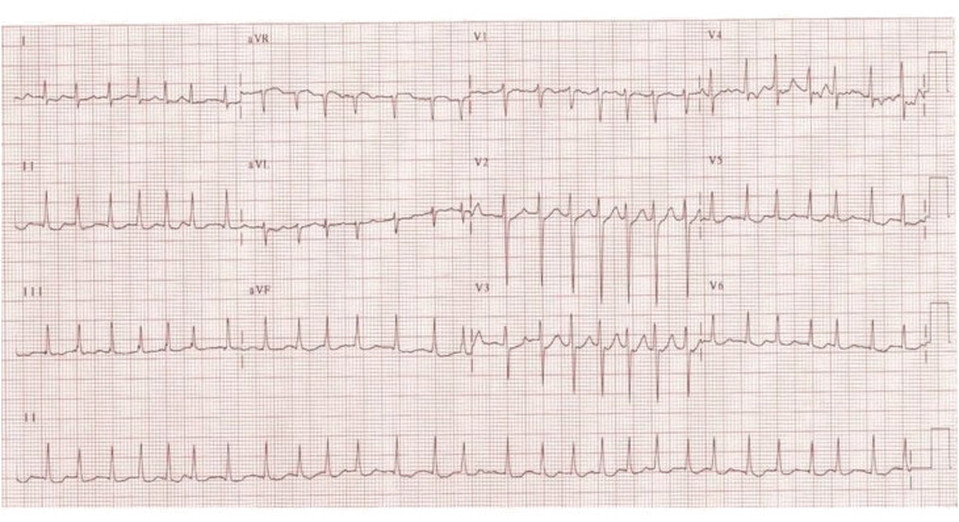
Question 1. What is the rate? (1 mark)
168 beats per minute (28 x 6).
Question 2. Is the rhythm regular or irregular? (1 mark)
Irregular
Question 3. What is the association of atrial beats to ventricular complexes? (1 mark)
There are no p waves seen.
Question 4. Comment on the PR and QT interval. (1 mark)
Must include: (0.5 marks each)
The PR interval cannot be calculated as there are no p waves seen.
The QT interval spans >50% of the RR interval it occurs in and therefore is prolonged to the naked eye.
Question 5. What is the axis? (1 mark)
Normal as I & aVF both have large positive deflections.
Question 6. Is there an interventricular conduction defect? Why or why not? (2 marks)
Must include (0.5 marks each(
No. The QRS is of normal duration (<0.12s).
Question 7. Comment on the ST segments. (1 mark)
Flattening of ST segments in II.
No indications seen for urgent reperfusion/no gross ischaemic change.
Question 8. What is the diagnosis? (2 marks)
Atrial fibrillation with rapid ventricular response.
168 beats per minute (28 x 6).
Question 2. Is the rhythm regular or irregular? (1 mark)
Irregular
Question 3. What is the association of atrial beats to ventricular complexes? (1 mark)
There are no p waves seen.
Question 4. Comment on the PR and QT interval. (1 mark)
Must include: (0.5 marks each)
The PR interval cannot be calculated as there are no p waves seen.
The QT interval spans >50% of the RR interval it occurs in and therefore is prolonged to the naked eye.
Question 5. What is the axis? (1 mark)
Normal as I & aVF both have large positive deflections.
Question 6. Is there an interventricular conduction defect? Why or why not? (2 marks)
Must include (0.5 marks each(
No. The QRS is of normal duration (<0.12s).
Question 7. Comment on the ST segments. (1 mark)
Flattening of ST segments in II.
No indications seen for urgent reperfusion/no gross ischaemic change.
Question 8. What is the diagnosis? (2 marks)
Atrial fibrillation with rapid ventricular response.
saq 7.
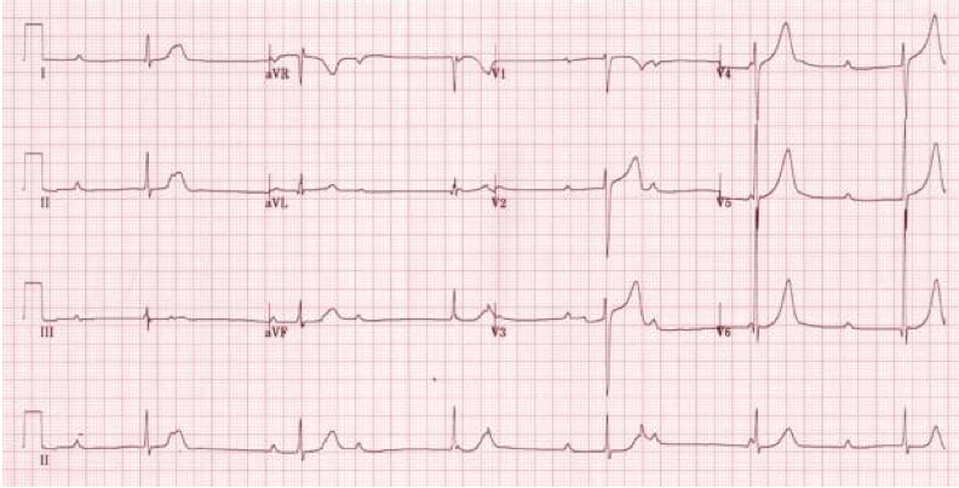
A 54 year old man presents with acute central chest pain that occurred while exercising. His pain has now gone away completely. On close questioning he describes a history of exertional dyspnoea and chest discomfort over the prior month.
His ECG on presentation is shown below. Assume standard calibration of the ECG (25mm/s and 10mm to 1mV).
His ECG on presentation is shown below. Assume standard calibration of the ECG (25mm/s and 10mm to 1mV).
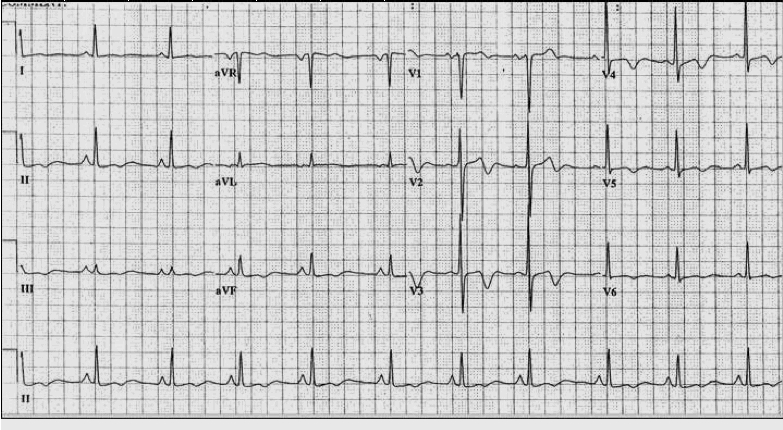
Question 1. Give 5 important normal findings on this ECG. (5 marks)
Must include:
- normal rate (60/min)
- 1:1 association of P & QRS complexes
Then 3 from:
- normal axis
- normal PR interval
- normal QRS duration
- normal QT interval
Question 2. What is the major electrocardiographic abnormality? (1 mark)
Deeply biphasic T waves in V2 - V4.
Question 3. What is the diagnosis? (1 mark)
Wellen's syndrome/proximal LAD lesion.
Question 4. Describe how the results of a troponin will affect your disposition of this patient. (3 marks)
Must include:
- disposition for this history and ECG is independent of troponin (1 mark)
- this patient requires an urgent PCI for LAD lesion (2 marks)
Must include:
- normal rate (60/min)
- 1:1 association of P & QRS complexes
Then 3 from:
- normal axis
- normal PR interval
- normal QRS duration
- normal QT interval
Question 2. What is the major electrocardiographic abnormality? (1 mark)
Deeply biphasic T waves in V2 - V4.
Question 3. What is the diagnosis? (1 mark)
Wellen's syndrome/proximal LAD lesion.
Question 4. Describe how the results of a troponin will affect your disposition of this patient. (3 marks)
Must include:
- disposition for this history and ECG is independent of troponin (1 mark)
- this patient requires an urgent PCI for LAD lesion (2 marks)
saq 8.
A 26 year old woman is brought to your emergency department after taking an overdose of an unknown susbtance. She has a prior history of depression and multiple overdoses in the past.
Her ECG on arrival is shown below.
Her ECG on arrival is shown below.
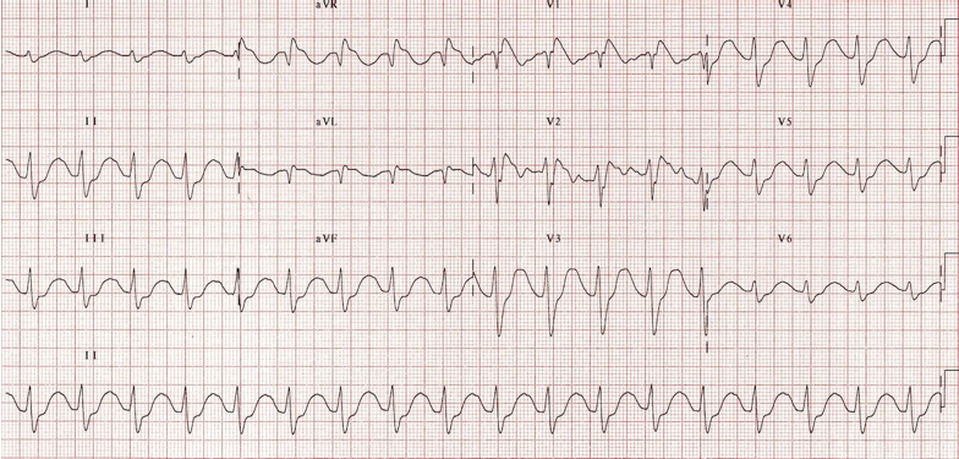
Question 1. What are the major abnormalities? (4 marks)
Tachycardia 108bpm
QRS >0.12s
Prolonged QT interval (>50% of RR interval)
Large R' in aVR
Question 2. Name four drugs from different classes which could cause this ECG and give an example of each. (4 marks)
Must include:
Tricyclic antidepressants (eg impiramine)
Plus any from:
Typical or atypical antipsychotics (eg droperidol or olanzapine
Anticonvulsants, specifically carbemazepine
Type 1A (Quinidine, procainamide, disopyramide) or 1C antiarrhythmics (flecainide)
Antimalarials (quinine, chloroquine, hydroxychloroquine)
Macrolides (erythmomycin, clarithromycin)
Question 3. What treatment will you administer as a matter of priority? (2 marks)
50ml NaHCO3 8.4% by slow IV push, repeated after 10-20 minutes for QT normalization.
Tachycardia 108bpm
QRS >0.12s
Prolonged QT interval (>50% of RR interval)
Large R' in aVR
Question 2. Name four drugs from different classes which could cause this ECG and give an example of each. (4 marks)
Must include:
Tricyclic antidepressants (eg impiramine)
Plus any from:
Typical or atypical antipsychotics (eg droperidol or olanzapine
Anticonvulsants, specifically carbemazepine
Type 1A (Quinidine, procainamide, disopyramide) or 1C antiarrhythmics (flecainide)
Antimalarials (quinine, chloroquine, hydroxychloroquine)
Macrolides (erythmomycin, clarithromycin)
Question 3. What treatment will you administer as a matter of priority? (2 marks)
50ml NaHCO3 8.4% by slow IV push, repeated after 10-20 minutes for QT normalization.
saq 9.
A 67 year old dialysis patient presents feeling weak and lethargic. He has missed his prior dialysis session because of a migraine.
His ECG on presentation to ED is shown below.
His ECG on presentation to ED is shown below.
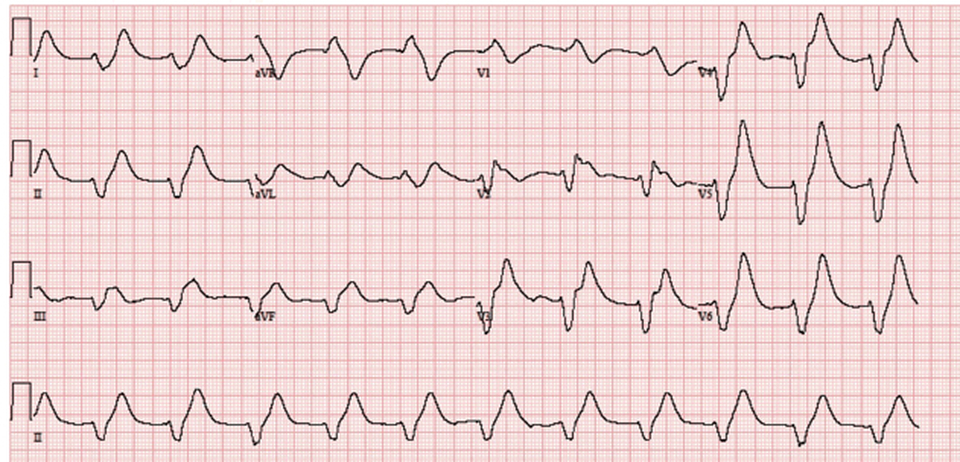
Question 1. What are the major abnormalities? (4 marks)
Must include:
short PR interval
wide QRS complex >0.12s
'northwest' axis
peaked t waves
Question 2. What is the likely diagnosis? (1 mark)
Critical Hyperkalaemia
Question 3. What treatments will you administer? (5 marks)
Must include (2 marks, must specify dose):
Either Calcium Gluconate 10% 10ml as a slow IV push OR Calcium Chloride 10% 10ml as slow IV push (either for 2 marks)
Also must include: (1 mark, must specify doses)
50ml 8.4% NaHCO3
10units IV actrapid plus 50ml 50% dextrose
Salbutamol 10-20mg via nebulizer
Must include:
short PR interval
wide QRS complex >0.12s
'northwest' axis
peaked t waves
Question 2. What is the likely diagnosis? (1 mark)
Critical Hyperkalaemia
Question 3. What treatments will you administer? (5 marks)
Must include (2 marks, must specify dose):
Either Calcium Gluconate 10% 10ml as a slow IV push OR Calcium Chloride 10% 10ml as slow IV push (either for 2 marks)
Also must include: (1 mark, must specify doses)
50ml 8.4% NaHCO3
10units IV actrapid plus 50ml 50% dextrose
Salbutamol 10-20mg via nebulizer
saq 10.
A 72 year old woman presents to your department with a history of sudden syncope while at church. The nurse looking after her brings you her ECG, which is shown below.
Question 1. What are the major abnormalities? (5 marks)
Must include:
1st degree heart block (PR >0.2s)
Leftward axis
QRS >0.12s
Deep S wave in V6/RBBB
T wave inversion III, aVF
Question 2. What is the diagnosis and its implications? (2 marks)
Trifasicular block - risk factor for development of high grade arrythmias.
Question 3.
30 minutes after arrival another ECG is taken as the patient is noted to be unconscious. The ECG is shown below. What are the two major abnormalities and what therefore does the ECG show? (3 marks)Question 3. 30 minutes after arrival another ECG is taken as the patient is noted to be unconscious. The ECG is shown below. What are the two major abnormalities and what therefore does the ECG show? (3 marks)
Must include:
1st degree heart block (PR >0.2s)
Leftward axis
QRS >0.12s
Deep S wave in V6/RBBB
T wave inversion III, aVF
Question 2. What is the diagnosis and its implications? (2 marks)
Trifasicular block - risk factor for development of high grade arrythmias.
Question 3.
30 minutes after arrival another ECG is taken as the patient is noted to be unconscious. The ECG is shown below. What are the two major abnormalities and what therefore does the ECG show? (3 marks)Question 3. 30 minutes after arrival another ECG is taken as the patient is noted to be unconscious. The ECG is shown below. What are the two major abnormalities and what therefore does the ECG show? (3 marks)
Must include:
- bradycardia rate 36
- complete dissociation of P and QRS complexes
- complete heart block
- bradycardia rate 36
- complete dissociation of P and QRS complexes
- complete heart block