SOLVE
A 48 yo male presents to the emergency department with palpitations. He has a past history of hypertension, for which he is on medications. His Heart rate is as below, BP 137/52, Sats 98% on room air and RR is 18. He is afebrile.
You are handed an ECG. See below:
(a) Describe the ECG and give a probable diagnosis
(b) List 4 differentials for this ECG
(c) List 4 features that you may use to diagnose Ventricular Tachycardia
(d) How would you treat this patient?
You are handed an ECG. See below:
(a) Describe the ECG and give a probable diagnosis
(b) List 4 differentials for this ECG
(c) List 4 features that you may use to diagnose Ventricular Tachycardia
(d) How would you treat this patient?
Whatever you do, have a system for looking at ECG's. I use my ECG in 20 seconds approach. It's up to you what you use.
Wide Complex tachycardias are one of the favourite ECG's, so know these well.
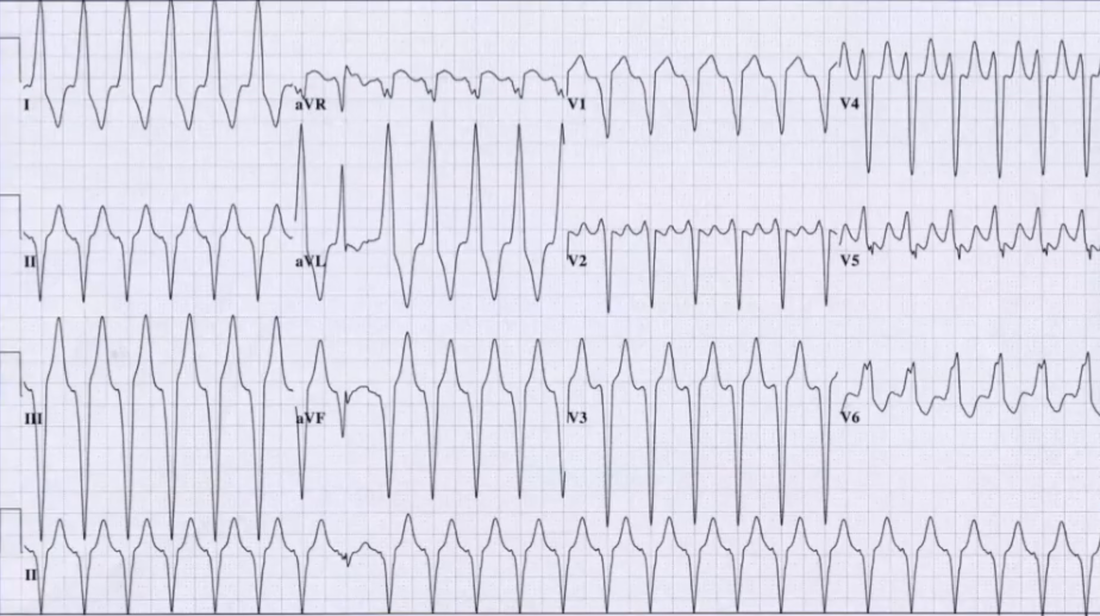
(a) This is a wide complex tachycardia. In detail:
Rate: 25 x 6 = 150
Rhythm: Are there P waves? Difficult to see
QRS: It is wide, in some leads approaching 160 and certainly >120ms.
Important to also mention what looks like a fusion beat
AXIS: Left
ST: Perhaps an elevation in aVR and some depression inV5
Intervals: QT looks prolonged, unable to comment on PR
Pacinf spikes: None to see
What else would you add?
This is a wide complex regular tachycardia, with a fusion beat. I would consider this to be Ventricular Tachycardia
(b)
(c)
You can use Brugada Criteria, or you can name others.
In this ECG:
Is the concordance? No
Is the RS interval > 100ms in any precordial lead?- difficult but probably No
Is there AV dissociation? No
Is the Rsr in V1? No Is there qR or QS in V6? No
Are there Capture or fusion beats? Yes
(d) Management in all patients is related to if the patient is stable or not.
If you are at all concerned cardiovert.
This patient is stable.
You may decide to treat as VT and sedate the patient- give drugs and doses ie., you might use ketamine 0.5mg/kg(35-40mg) and propofol of 50-100mg, or just propofol. Use 100J
What drugs ould you use?
Amiodarone?
Adenosine.
It's interesting in that this is in fact a case of WPW with SVT. Following cardioversion the patient's ECG was as below:
Wide Complex tachycardias are one of the favourite ECG's, so know these well.
(a) This is a wide complex tachycardia. In detail:
Rate: 25 x 6 = 150
Rhythm: Are there P waves? Difficult to see
QRS: It is wide, in some leads approaching 160 and certainly >120ms.
Important to also mention what looks like a fusion beat
AXIS: Left
ST: Perhaps an elevation in aVR and some depression inV5
Intervals: QT looks prolonged, unable to comment on PR
Pacinf spikes: None to see
What else would you add?
This is a wide complex regular tachycardia, with a fusion beat. I would consider this to be Ventricular Tachycardia
(b)
- Ventricular tachycardia
- SVT with bundle branch block (LBBB or RBBB)
- SVT with WPW
- Na Channel Blockade
(c)
You can use Brugada Criteria, or you can name others.
In this ECG:
Is the concordance? No
Is the RS interval > 100ms in any precordial lead?- difficult but probably No
Is there AV dissociation? No
Is the Rsr in V1? No Is there qR or QS in V6? No
Are there Capture or fusion beats? Yes
(d) Management in all patients is related to if the patient is stable or not.
If you are at all concerned cardiovert.
This patient is stable.
You may decide to treat as VT and sedate the patient- give drugs and doses ie., you might use ketamine 0.5mg/kg(35-40mg) and propofol of 50-100mg, or just propofol. Use 100J
What drugs ould you use?
Amiodarone?
Adenosine.
It's interesting in that this is in fact a case of WPW with SVT. Following cardioversion the patient's ECG was as below:
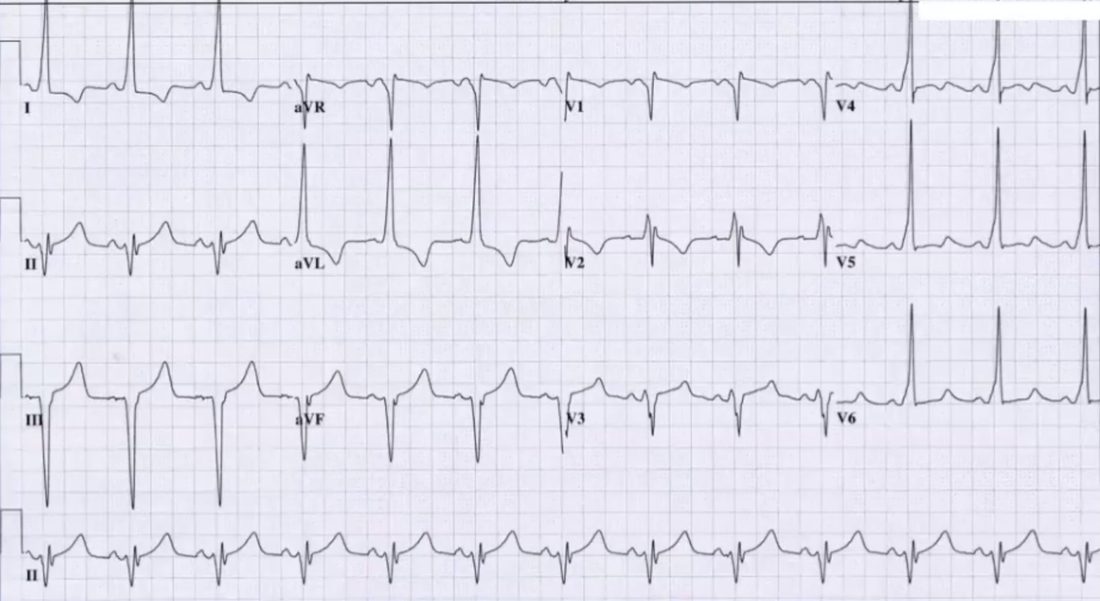
ECG from Amal Mattu lectures.