MODULE eight short answer questions.
saq 1.
An excerpt of the Australian resuscitation council guideline for advanced life support is shown below.
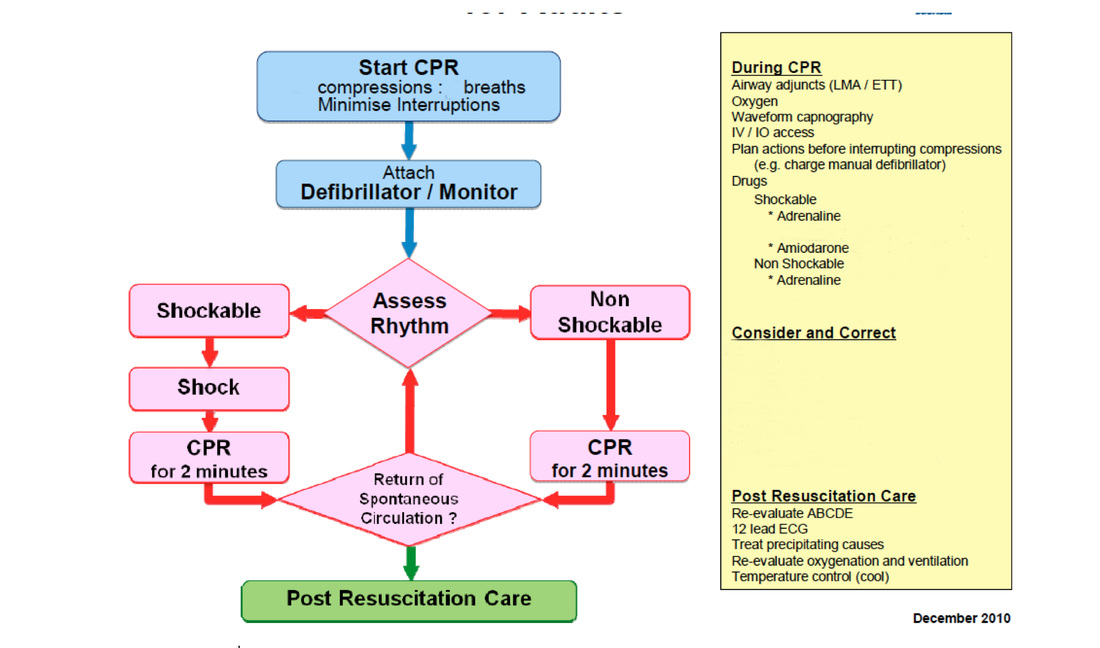
Question 1. (4 marks)
What is the difference between a “shockable” and “non-shockable” rhythm? Give 2 examples of a shockable rhythm.
Must include: (2 marks)
Shockable rhythms are those likely to respond to defibrillation.
A non shockable rhythm has a relatively normal electrical complex and therefore does not respond to defibrillation.
Shockable rhythms: (1 mark each must specify "pulseless" with VT)
-VF
-Pulseless VT
Question 2. (1mark)
What is the ratio of compressions to breaths for CPR?
Must include:
30 compressions: 2 breaths
Question 3. (4 marks)
What doses and when should drugs be given for a “shockable rhythm”?
Must include:
Adrenaline 1mg after 2nd shock
then every 2nd loop
Amiodarone 300mg after 3rd shock
can be given a further 150mg bolus after another 2 cycles
Note, the above answer is based on the existing ARC guidelines (the basis of the question). This becomes very confusing in terms of reconciling the 2015 ILCOR guidelines, the extant ARC guidelines and what the hell to write in the actual exam.
The executive summary of the 2015 ILOR guidelines (pg 17/18) states that for a shockable rhythm:
- give 1mg of adrenaline every 3-5 minutes
- give amiodarone 300mg IV after the third shock, with a further 150mg after the 5th shock if VF persists.
Thus we would suggest that although the first answer above is technically correct, perhaps a safer way of answering would be to use the second answer statement, which covers the first eventuality well and removes a lot of problematic ambiguity by relating adrenaline to time rather than cycles.
Thanks Dr Moulden for the astute observation of the discrepancies between the two statements!
Question 4. (2 marks)
What dose of adrenaline should be given when in a non-shockable rhythm? (1 mark)
Adrenaline 1mg immediately
and then every second loop
Question 5. (1 mark)
What is the ratio of compressions to ventilations in children?
Must include:
-15 compressions to 2 breaths
Question 6. (6 marks)
Give 6 reversible causes of non-shockable arrests in adults.
Must include 6 from (6 marks each):
-hypoxia
-hypovolaemia
-hyper/hypokalaemia
-hypo/hyperthermia
-tension pneumothorax
-tamponade
-thrombosis (pe/cardiac)
-toxins
What is the difference between a “shockable” and “non-shockable” rhythm? Give 2 examples of a shockable rhythm.
Must include: (2 marks)
Shockable rhythms are those likely to respond to defibrillation.
A non shockable rhythm has a relatively normal electrical complex and therefore does not respond to defibrillation.
Shockable rhythms: (1 mark each must specify "pulseless" with VT)
-VF
-Pulseless VT
Question 2. (1mark)
What is the ratio of compressions to breaths for CPR?
Must include:
30 compressions: 2 breaths
Question 3. (4 marks)
What doses and when should drugs be given for a “shockable rhythm”?
Must include:
Adrenaline 1mg after 2nd shock
then every 2nd loop
Amiodarone 300mg after 3rd shock
can be given a further 150mg bolus after another 2 cycles
Note, the above answer is based on the existing ARC guidelines (the basis of the question). This becomes very confusing in terms of reconciling the 2015 ILCOR guidelines, the extant ARC guidelines and what the hell to write in the actual exam.
The executive summary of the 2015 ILOR guidelines (pg 17/18) states that for a shockable rhythm:
- give 1mg of adrenaline every 3-5 minutes
- give amiodarone 300mg IV after the third shock, with a further 150mg after the 5th shock if VF persists.
Thus we would suggest that although the first answer above is technically correct, perhaps a safer way of answering would be to use the second answer statement, which covers the first eventuality well and removes a lot of problematic ambiguity by relating adrenaline to time rather than cycles.
Thanks Dr Moulden for the astute observation of the discrepancies between the two statements!
Question 4. (2 marks)
What dose of adrenaline should be given when in a non-shockable rhythm? (1 mark)
Adrenaline 1mg immediately
and then every second loop
Question 5. (1 mark)
What is the ratio of compressions to ventilations in children?
Must include:
-15 compressions to 2 breaths
Question 6. (6 marks)
Give 6 reversible causes of non-shockable arrests in adults.
Must include 6 from (6 marks each):
-hypoxia
-hypovolaemia
-hyper/hypokalaemia
-hypo/hyperthermia
-tension pneumothorax
-tamponade
-thrombosis (pe/cardiac)
-toxins
saq 2. (FOLLOWS ON INTO SAQ 3).
A 78 year old man presents to your emergency department with the ambulance after an episode of syncope. On arrival his vital signs are
HR 54 /min
BP 112/65 mmHg
RR 18 /min
T 37.1 oC
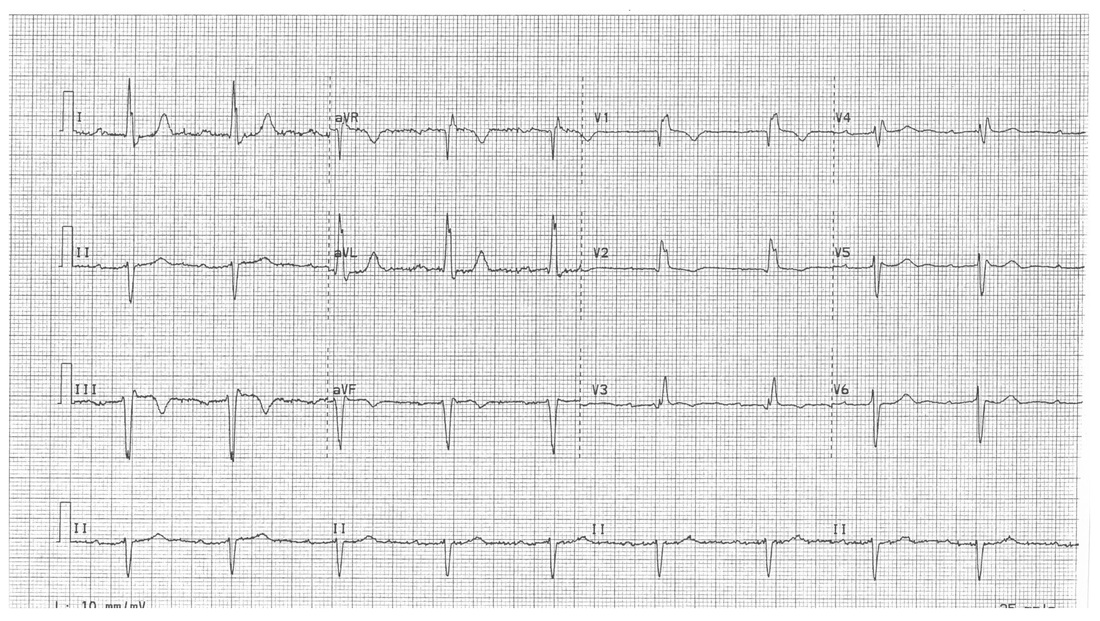
His ECG on arrival is shown below.
HR 54 /min
BP 112/65 mmHg
RR 18 /min
T 37.1 oC
His ECG on arrival is shown below.
Question 1. (5 marks)
What give three abnormalities seen on the ECG, the underlying diagnosis and are the implications for this patient's presentation?
Must include
-1st degree heart block/prolonged PR
-leftward axis
-RBBB pattern
This gives a diagnosis of trifasicular block
This ECG is high risk for a high grade heart block.
What give three abnormalities seen on the ECG, the underlying diagnosis and are the implications for this patient's presentation?
Must include
-1st degree heart block/prolonged PR
-leftward axis
-RBBB pattern
This gives a diagnosis of trifasicular block
This ECG is high risk for a high grade heart block.
Question 2.
The patient suffers an episode of syncope in the department. His vital signs are retaken:
HR 35 /min
BP 72/38 /min
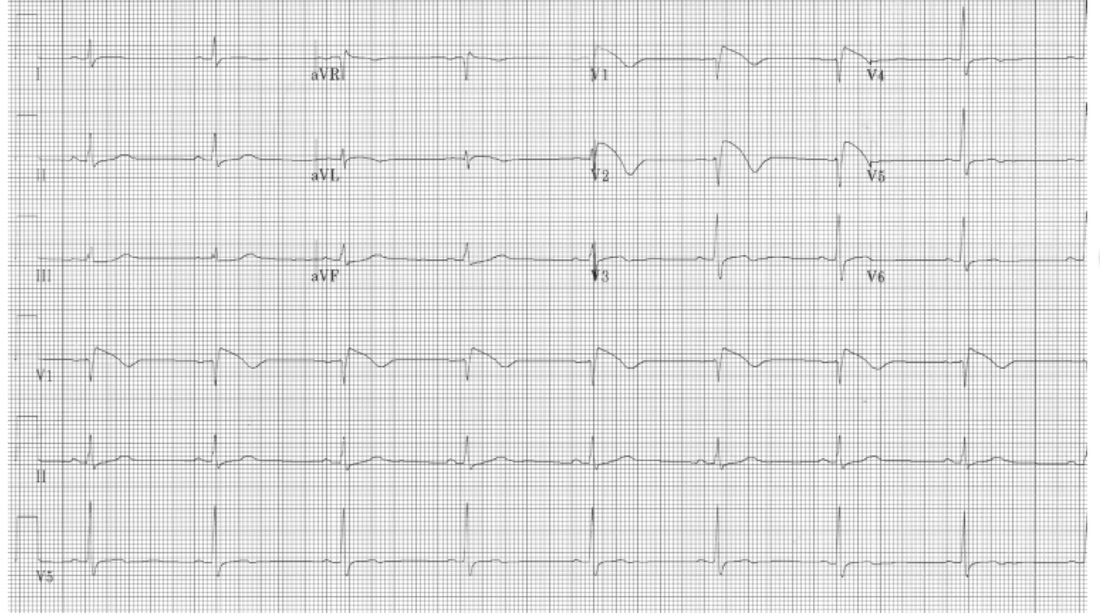
A repeat ECG is shown below. Give two abnormalities shown by the ECG and the diagnosis.
The patient suffers an episode of syncope in the department. His vital signs are retaken:
HR 35 /min
BP 72/38 /min
A repeat ECG is shown below. Give two abnormalities shown by the ECG and the diagnosis.
Must include:
-dissociation of p waves from QRS complexes
-wide QRS complexes
diagnosis: complete heart block
Question 3. (4 marks)
Give 2 medications you could administer in this situation and the appropriate doses?
Must include any 2 of (1 mark for drug and 1 mark for correct dose):
-atropine 600mcg stat bolus
-adrenaline either 20-50mcg IV stat or infusion titrated upwards from a reasonable dose (eg 2mcg/min)
-isoprenaline infusion titrated upwards from a resonable dose (2-5mcg/min)
-dissociation of p waves from QRS complexes
-wide QRS complexes
diagnosis: complete heart block
Question 3. (4 marks)
Give 2 medications you could administer in this situation and the appropriate doses?
Must include any 2 of (1 mark for drug and 1 mark for correct dose):
-atropine 600mcg stat bolus
-adrenaline either 20-50mcg IV stat or infusion titrated upwards from a reasonable dose (eg 2mcg/min)
-isoprenaline infusion titrated upwards from a resonable dose (2-5mcg/min)
saq 3. (FOLLOWS FROM SAQ 2.)
The patient from SAQ 2 has does not respond to the drugs you administer.
Question 1.
What treatment will you now administer?
Must include:
- transthoracic pacing. (1 mark)
Question 2.
Describe your method for doing this. (5 marks)
Must include:
-use of pads and leads placed concurrently
-administration of appropriate sedation
-selection of “synchronised” mode
-administration of current (usually ~80mA) ensuring electrical and mechanical capture
-reduction of current to “capture threshold” and then increase to 10% above this
Question 3. (7 marks)
Select pathology results for the patient are shown below. Give 3 major abnormalities and give 2 treatments you will commence.
Na+ 140 mmol/L
K+ 6.1 mmol/L
Cl- 100 mmol/L
Urea 13.6 mmol/L
Creatinine 146 mmol/L
digoxin 12 ng/ml
Must include:
Abnormalities: (must
-acute renal failure (1 mark)
-hyperkalaemia (1 mark)
-elevated digoxin level (1 mark)
Treatment: (4 marks)
-administration of digoxin Fab fragments : 2 vials over 30 minutes titrated to effect
-insulin 10IU actrapid and dextrose 25g for hyperkalaemia
Question 1.
What treatment will you now administer?
Must include:
- transthoracic pacing. (1 mark)
Question 2.
Describe your method for doing this. (5 marks)
Must include:
-use of pads and leads placed concurrently
-administration of appropriate sedation
-selection of “synchronised” mode
-administration of current (usually ~80mA) ensuring electrical and mechanical capture
-reduction of current to “capture threshold” and then increase to 10% above this
Question 3. (7 marks)
Select pathology results for the patient are shown below. Give 3 major abnormalities and give 2 treatments you will commence.
Na+ 140 mmol/L
K+ 6.1 mmol/L
Cl- 100 mmol/L
Urea 13.6 mmol/L
Creatinine 146 mmol/L
digoxin 12 ng/ml
Must include:
Abnormalities: (must
-acute renal failure (1 mark)
-hyperkalaemia (1 mark)
-elevated digoxin level (1 mark)
Treatment: (4 marks)
-administration of digoxin Fab fragments : 2 vials over 30 minutes titrated to effect
-insulin 10IU actrapid and dextrose 25g for hyperkalaemia
saq 4.
A 17 year old male presents after an episode of syncope on the soccer pitch. He has no medical history of note. On presentation to the emergency department his vital signs are:
HR 67 /min
BP 110/65 mmHg
RR 18 /min
Sats 99% RA
T 37.2 oC
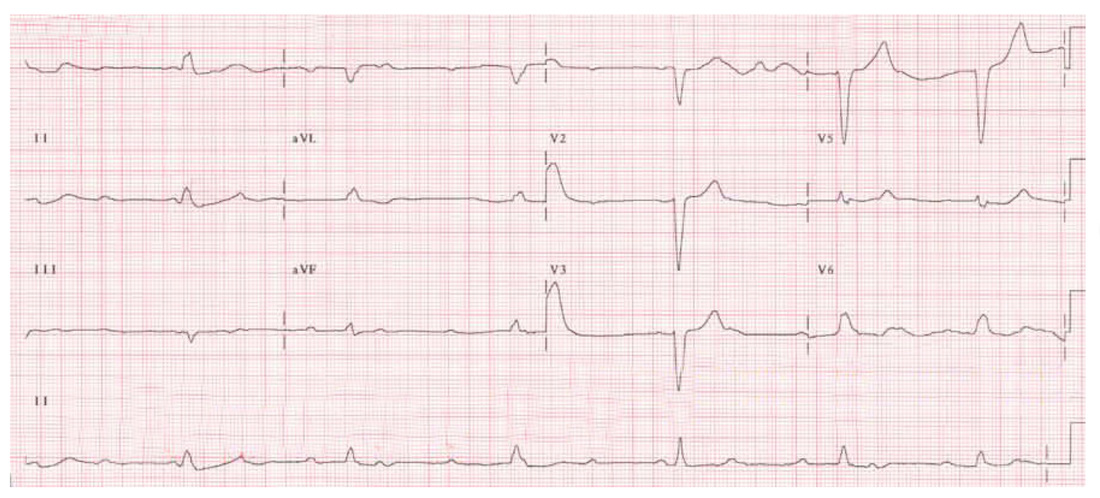
He is placed in the subacute area and an ECG is taken.
HR 67 /min
BP 110/65 mmHg
RR 18 /min
Sats 99% RA
T 37.2 oC
He is placed in the subacute area and an ECG is taken.
Question 1. (3 marks)
What is the major abnormality seen on the ECG and what diagnosis is suggested?
Must include:
-significant downsloping (“coved”) ST elevation in V1 & V2
-associated with t wave inversion
-in combination with syncope this suggests Brugada syndrome.
Question 2. (1 mark)
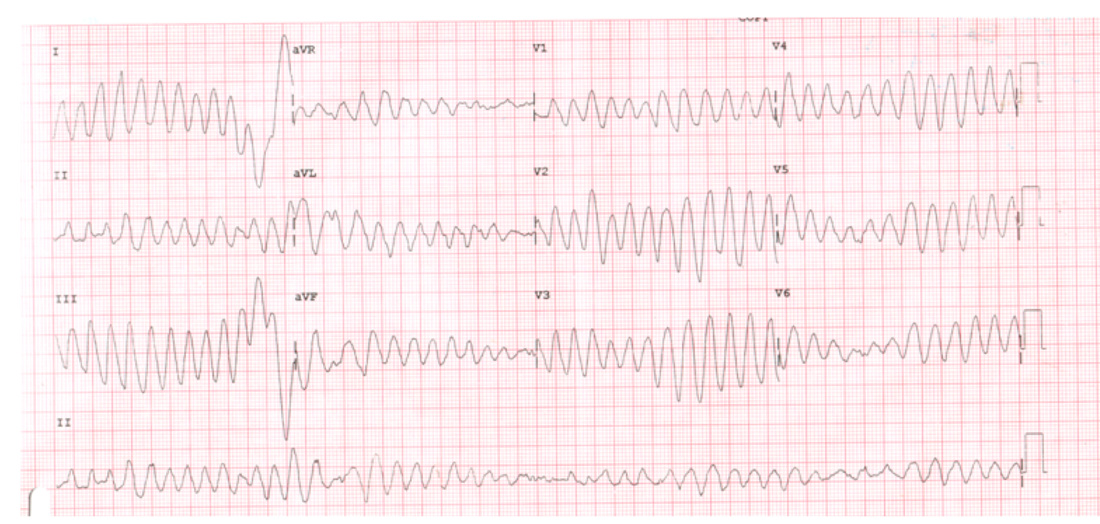
The nurse looking after the patient reports another episode of syncope in the department, and tells you he has run a repeat ECG which is shown below. What does the ECG show?
What is the major abnormality seen on the ECG and what diagnosis is suggested?
Must include:
-significant downsloping (“coved”) ST elevation in V1 & V2
-associated with t wave inversion
-in combination with syncope this suggests Brugada syndrome.
Question 2. (1 mark)
The nurse looking after the patient reports another episode of syncope in the department, and tells you he has run a repeat ECG which is shown below. What does the ECG show?
Question 3. (2 marks)
The patient is awake, with a blood pressure of 110 systolic.
What treatment will you administer?
Must include: (1 mark each)
- bolus dose magnesium 20mmol over 10-15 minutes
-then 40mmol infusion over 4-6 hours
Question 4. (5 marks)
Shortly after treating this patinet, the ambulance brings in a 56 year old patient who has ROSC after a cardiac arrest in the community. He has had 5 minutes of CPR and responded to a 200J for ventricular fibrillation. The patient has been intubated on scene. On arrival he is sedated, paralyzed and his vital signs are:
HR 104 /min
BP 95/60 mmHg
RR 16
Sats 100% 100% O2
T 37.4 oC
Give 5 treatment priorities you now have for this patient?
Must include:
-evaluation for cause of arrest: MI, PE, electrolyte disturbance and correction of any issue
-cooling to 36 degrees
-early transfer to cardiac cath lab in absence of any other clear precipitant
Plus other reasonable statements such as:
-ensure optimal ventilation
-NGT to decompress stomach and assist ventilation
-contact family with updated info
The patient is awake, with a blood pressure of 110 systolic.
What treatment will you administer?
Must include: (1 mark each)
- bolus dose magnesium 20mmol over 10-15 minutes
-then 40mmol infusion over 4-6 hours
Question 4. (5 marks)
Shortly after treating this patinet, the ambulance brings in a 56 year old patient who has ROSC after a cardiac arrest in the community. He has had 5 minutes of CPR and responded to a 200J for ventricular fibrillation. The patient has been intubated on scene. On arrival he is sedated, paralyzed and his vital signs are:
HR 104 /min
BP 95/60 mmHg
RR 16
Sats 100% 100% O2
T 37.4 oC
Give 5 treatment priorities you now have for this patient?
Must include:
-evaluation for cause of arrest: MI, PE, electrolyte disturbance and correction of any issue
-cooling to 36 degrees
-early transfer to cardiac cath lab in absence of any other clear precipitant
Plus other reasonable statements such as:
-ensure optimal ventilation
-NGT to decompress stomach and assist ventilation
-contact family with updated info
saq 5.
A 68 year old woman presents with a high fever and dyspnoea. She describes having a productive cough for the preceding 3 days. She has a history of rheumatoid arthritis treated with methotrexate.
On arrival her vital signs are:
HR 119 /min
BP 86/42 mmHg
RR 36 /min
Sats 92% 6L O2
Question 1. (4 marks)
How will you clinically assess the volume status of this patient?
Must include:
-capillary refill time
-JVP 3-4cm
plus other reasonable metrics
-postural drop >10mmHg
-dry mucous membranes
-tissue turgor increased
-etc
A venous gas is taken in the resuscitation room and the results are shown below.
pH 7.25
pCO2 32 mmHg
HCO3- 16 mmol/L
BE -8
Na+ 132 mmol/L
K+ 5.5 mmol/L
Cl- 100 mmol/L
Urea 12.5 mmol/L
Cr 130 umol/L
Lactate 4.6 mmol/L
Question 2. (3 marks)
Give 3 acid/base disturbances that are present.
Must include:
RAGMA
NAGMA
Compensatory respiratory alkalosis
Question 3. (3 marks)
Provide 3 calculations to support your answer.
Must include:
Anion gap = 132 - (100+16) = 16 HIGH (RAGMA)
Delta Ratio = (16-12)/(24-16) = 4/8 = 0.5. Implies concurrent NAGMA
Expect CO2 = 1.5 x 16 + 8 = 32mmHg APPROPRIATE COMPENSATION
Question 4. (3 marks)
Give 3 other abnormalities seen on the blood gas.
Must include:
Raised renal indices (high urea/creatinine)
Mild hyperkalaemia, approproriate for pH (expect 5 + 1.5 x 0.5 = 5.75mmol/L)
Mild hyponatraemia
Question 5. (2 marks)
Clinically the patient is anuric. Provide an explanation for this based on the VBG and a calculation to support your answer.
The urea to creatinine ratio is approximately 100, which implies pre-renal failure, likely hypovolaemia/dehydration from septic shock
Question 6. (3 marks)
What initial management will you institute?
-fluid resuscitation 20ml/kg - 40ml/kg for SBP >90mmHg cap refill 2sec
-early broad spectrum antibiotics: pip/taz 4.5g (0.5 mark) & gentamicin 5-7mg/kg (0.5 mark)
- increase O2 for sats >95%
Question 7. (2 marks)
After your initial treatment remains hypotensive with a blood pressure of 82 systolic. What further management will you institute?
Must include
-further fluid bolus to endpoint above or JVP 4cm, CVP 8-10mmHg
-institution of inotropes: noradrenaline or adrenaline 10mcg/min for MAP >65mmHg
On arrival her vital signs are:
HR 119 /min
BP 86/42 mmHg
RR 36 /min
Sats 92% 6L O2
Question 1. (4 marks)
How will you clinically assess the volume status of this patient?
Must include:
-capillary refill time
-JVP 3-4cm
plus other reasonable metrics
-postural drop >10mmHg
-dry mucous membranes
-tissue turgor increased
-etc
A venous gas is taken in the resuscitation room and the results are shown below.
pH 7.25
pCO2 32 mmHg
HCO3- 16 mmol/L
BE -8
Na+ 132 mmol/L
K+ 5.5 mmol/L
Cl- 100 mmol/L
Urea 12.5 mmol/L
Cr 130 umol/L
Lactate 4.6 mmol/L
Question 2. (3 marks)
Give 3 acid/base disturbances that are present.
Must include:
RAGMA
NAGMA
Compensatory respiratory alkalosis
Question 3. (3 marks)
Provide 3 calculations to support your answer.
Must include:
Anion gap = 132 - (100+16) = 16 HIGH (RAGMA)
Delta Ratio = (16-12)/(24-16) = 4/8 = 0.5. Implies concurrent NAGMA
Expect CO2 = 1.5 x 16 + 8 = 32mmHg APPROPRIATE COMPENSATION
Question 4. (3 marks)
Give 3 other abnormalities seen on the blood gas.
Must include:
Raised renal indices (high urea/creatinine)
Mild hyperkalaemia, approproriate for pH (expect 5 + 1.5 x 0.5 = 5.75mmol/L)
Mild hyponatraemia
Question 5. (2 marks)
Clinically the patient is anuric. Provide an explanation for this based on the VBG and a calculation to support your answer.
The urea to creatinine ratio is approximately 100, which implies pre-renal failure, likely hypovolaemia/dehydration from septic shock
Question 6. (3 marks)
What initial management will you institute?
-fluid resuscitation 20ml/kg - 40ml/kg for SBP >90mmHg cap refill 2sec
-early broad spectrum antibiotics: pip/taz 4.5g (0.5 mark) & gentamicin 5-7mg/kg (0.5 mark)
- increase O2 for sats >95%
Question 7. (2 marks)
After your initial treatment remains hypotensive with a blood pressure of 82 systolic. What further management will you institute?
Must include
-further fluid bolus to endpoint above or JVP 4cm, CVP 8-10mmHg
-institution of inotropes: noradrenaline or adrenaline 10mcg/min for MAP >65mmHg