MODULE 10: penetrating neck trauma, chest trauma and abdominal trauma.
[the trauma block]
You'll be happy to hear that this week is going to be a bit less intense than last week. To be honest, the really avant garde trauma stuff is not what tends to be on the exam. You need to be able to read CTs and X-rays, discuss common problems sensibly and be safe. Most of the major trauma stuff is about application of knowledge paradigms (hypotensive resuscitation, massive transfusion, damage control etc) rather than knowing the difference between a grade x and grade y splenic tear.
We have some more EMCORE videos for you below. We would also recommend that you pay particular attention to Cameron's chapters on thoracic and abdominal trauma to pick up all the minor factoids you need to be able to mention.
We have some more EMCORE videos for you below. We would also recommend that you pay particular attention to Cameron's chapters on thoracic and abdominal trauma to pick up all the minor factoids you need to be able to mention.
watch.
|
|
|
READ
We want to reiterate our points about making sure you're up with Cameron and Dunn this week. Although trauma is a dynamic area in real life, knowing the party line for the exam is really important.
For those who are interested here are some good pages with images to look at on pneumothorax, tension pneumothorax, haemothorax and flail chest.
For those who are interested here are some good pages with images to look at on pneumothorax, tension pneumothorax, haemothorax and flail chest.
Below are some articles for you: (both 2 and 3 are really for interest only if you have time...)
1. A brief (but rather good) overview of an up to date approach to neck trauma. Worth a look.
1. A brief (but rather good) overview of an up to date approach to neck trauma. Worth a look.
| neck_no_zone.pdf |
2. A review of ED thoracotomy practice
| ed_thoracotomy_review_1.pdf |
3. The original REBOA article
solve.
This week we are returning the the arterial blood gas. The gas below is not strictly speaking related to trauma, but it is from a real exam, and with the next face to face approaching we wanted to maintain the momentum with interpreting ABGs.
We're going to do this in the old school style - the aim is to see how much you can get out of an arterial blood gas in as little time as possible.
Give yourself 6 minutes (you have this in the real exam) and have a look at the ABG below. Your task - should you choose to accept it - is to describe and interpret the gas. Specifically give all the disturbances possible, perform all the calculations and give a likely diagnosis.
Ready? GO!
A 30 year old man presents to your ED with a history of increasing weakness for 24 hours. An arterial blood gas and electrolytes are performed.
We're going to do this in the old school style - the aim is to see how much you can get out of an arterial blood gas in as little time as possible.
Give yourself 6 minutes (you have this in the real exam) and have a look at the ABG below. Your task - should you choose to accept it - is to describe and interpret the gas. Specifically give all the disturbances possible, perform all the calculations and give a likely diagnosis.
Ready? GO!
A 30 year old man presents to your ED with a history of increasing weakness for 24 hours. An arterial blood gas and electrolytes are performed.
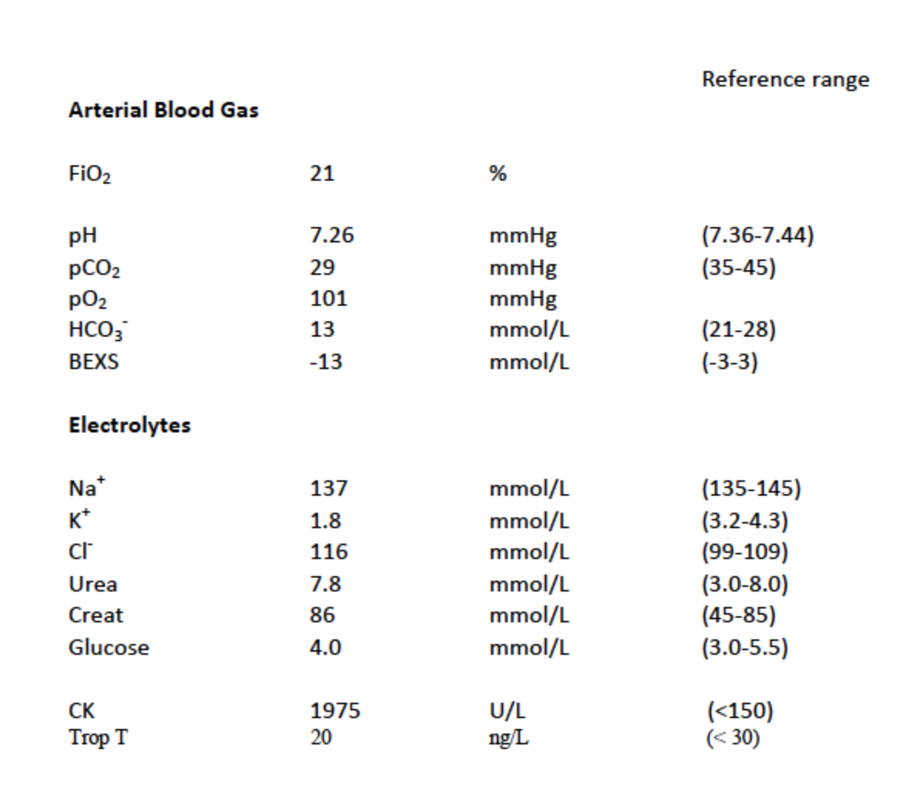
Describe and interpret the results. (100%)
write.
To focus on the ABG this week we want to to write the following:
1. An SAQ featuring an ABG as a prop on the week's topics
2. 5 MCQs incorporating the week's topics.
Up on the VSG as usual please. Writing an ABG is a very good way to start understanding them.
1. An SAQ featuring an ABG as a prop on the week's topics
2. 5 MCQs incorporating the week's topics.
Up on the VSG as usual please. Writing an ABG is a very good way to start understanding them.