MODULE Seven short answer questions.
saq 1.
An 85 year old female is found by the ambulance after not being seen for 24 hours. She has been found lying naked on her bathroom floor, with an altered level of consciousness. The ambulance report that the window was open and the shower was on.
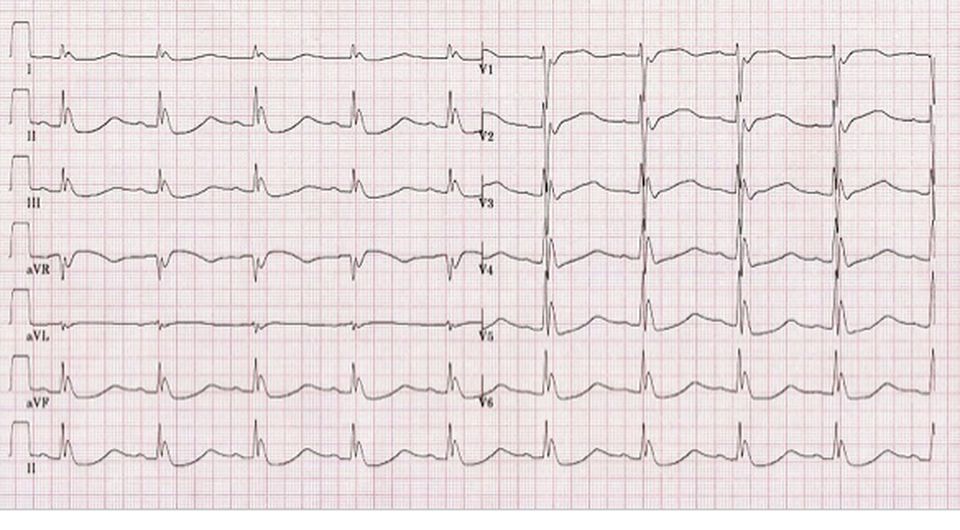
Her arrival ECG is shown below.
Question 1.
What does the ECG show? Assume standard 25mm/s calibration. (4 marks)
Answer must include:
- Bradycardia HR 45
- 1st degree heart block
- Prolonged QT interval
- Pronounced Osbourne waves
Question 2.
What is the differential diagnosis? (3 marks)
Must include:
Hypothermia
Plus any other of
Question 3.
List six investigations you will perform on this patient and the indications for each. (6 marks)
What does the ECG show? Assume standard 25mm/s calibration. (4 marks)
Answer must include:
- Bradycardia HR 45
- 1st degree heart block
- Prolonged QT interval
- Pronounced Osbourne waves
Question 2.
What is the differential diagnosis? (3 marks)
Must include:
Hypothermia
Plus any other of
- Hypocalcaemia/calcium disturbance
- Subarachoid haemorrhage
- Idiopathic VF
Question 3.
List six investigations you will perform on this patient and the indications for each. (6 marks)
|
INVESTIGATION
1. 2. 3. 4. 5. 6. |
INDICATION
1. 2. 3. 4. 5. 6. |
Must include:
BSL: ?cause for altered LOC
UEC: renal indices and K+
VBG lactate: pH plus ?RAGMA/sepsis
CMP: check Ca lvl in likely rhabdomyolysis
CK: long lie/rhabdomylosis
Plus any of
BSL: ?cause for altered LOC
UEC: renal indices and K+
VBG lactate: pH plus ?RAGMA/sepsis
CMP: check Ca lvl in likely rhabdomyolysis
CK: long lie/rhabdomylosis
Plus any of
- m/c/s urine ?UTI
- CXR ?aspiration
- CT brain (ALOC)
- FBC – anaemia/sepsis
- BCs if sepsis suspected
saq 2.
A 17 year old male is brought to your emergency department during winter. The local river has frozen over. The patient had been drinking at the local pub with friends and dived off a bridge into the river. He ran into trouble, and had a prolonged immersion time. There is no overt trauma.
On arrival the patient’s vital signs are:
HR 46
BP 85/45
RR 12
Sats 99%
T 28.6 oC
Question 1.
Give three principles you will apply to your management of this patient, and the rationale for each. (6 marks)
On arrival the patient’s vital signs are:
HR 46
BP 85/45
RR 12
Sats 99%
T 28.6 oC
Question 1.
Give three principles you will apply to your management of this patient, and the rationale for each. (6 marks)
|
PRINCIPLE.
1. Application of active rewarming 2. Minimize handling/intervention 3. Aim for rapid rise above 30oC and then steady rewarming afterwards |
RATIONALE.
1. This patient is profoundly hypothermic and will require higher level rewarming techniques 2. Classically these promote arrythmogenesis in the hypothermic patient 3. Risk of dysrhythmia is greatest below 30o, and plateaus after this. |
Question 2.
Give 5 methods of rewarming this patient. (5 marks)
Must include: (1 mark each)
Note, both thoracic and peritoneal lavage would be considered extreme techniques and probably NOT appropriate for this clinical presentation.
Question 3.
Give two criteria for calling off cardiac resuscitation in a hypothermic patient?
Must include thematically:
Plus either of (1 mark each):
Give 5 methods of rewarming this patient. (5 marks)
Must include: (1 mark each)
- Removal of wet clothes
- Use of rewarming blanket/warm packs over axillae/groin
- Administration of warmed IV fluid via fluid warmer
- Administration of humidified oxygen
- Gastric lavage with warm fluid
- 3 way irrigation of bladder with warmed fluid
Note, both thoracic and peritoneal lavage would be considered extreme techniques and probably NOT appropriate for this clinical presentation.
Question 3.
Give two criteria for calling off cardiac resuscitation in a hypothermic patient?
Must include thematically:
- Temperature above 32 degrees and no signs of life/asystole
Plus either of (1 mark each):
- Obvious unsurvivable trauma
- Serum K+ >10
saq 3.
Question 1. (9 marks)
Fill in the following table with the relevant features of hypothermia.
Fill in the following table with the relevant features of hypothermia.
|
MILD HYPOTHERMIA MODERATE HYPOTHERMIA SEVERE HYPOTHERMIA |
TEMPERATURE RANGE
32 - 35 28 - 32 <28 |
CLINICAL FEATURES
Shivering, confusion/dysarthria, diuresis Loss of shivering, severe confusion, dilated/poorly responsible pupils Unresponsiveness/coma, pulmonary oedema |
CARDIAC FEATURES
Either tachy or brady-arrythmia Bradycardia, J waves Bradycardia/slow AF Refractory VF |
Question 2. (2 marks)
Give 2 methods of invasive temperature monitoring which can be used in the emergency department. (1 mark)
Must include:
Give 2 methods of invasive temperature monitoring which can be used in the emergency department. (1 mark)
Must include:
- IDC with temperature probe
- Nasogastrically inserted temperature probe.
saq 4.
A 92 year old female is brought into the emergency department after being found unconscious by her neighbour. She was last seen 36 hours previously.
On arrival in the ED it is noted that she is asystolic, and CPR is commenced. Her temperature is noted to be 31oC and her pupils are fixed and dilated.
An urgent arterial blood gas is taken via femoral stab during the initial phase of the resuscitation and results are shown below.
pH 7.02
PO2 25 mmHg
PCO2 88 mmHg
HCO3- 2 mmol/L
Lactate 10.6 mmol/L
Na+ 141 mmol/L
K+ 10.2 mmol/L
Cl- 100 mmol/L
Question 1.
What are the major abnormalities? (5 marks)
Must include:
Severe acidaemia
Severe hypocapnoea
Severe hypoxia
Profound hyperlactataemia
Critical Hyperkalaemia
Question 2. (1 mark)
What is the anion gap?
Must include: 39 (no K+ included) or 29 (K+ included)
Question 3. (2 marks)
What management will you institute?
Must include:
Question 4. (2 marks)
A member of your team objects to cessation of resuscitation on the basis of the patient’s temperature, suggesting that the patient should be actively rewarmed before she can be pronounced dead. How will you respond?
Must include thematically:
On arrival in the ED it is noted that she is asystolic, and CPR is commenced. Her temperature is noted to be 31oC and her pupils are fixed and dilated.
An urgent arterial blood gas is taken via femoral stab during the initial phase of the resuscitation and results are shown below.
pH 7.02
PO2 25 mmHg
PCO2 88 mmHg
HCO3- 2 mmol/L
Lactate 10.6 mmol/L
Na+ 141 mmol/L
K+ 10.2 mmol/L
Cl- 100 mmol/L
Question 1.
What are the major abnormalities? (5 marks)
Must include:
Severe acidaemia
Severe hypocapnoea
Severe hypoxia
Profound hyperlactataemia
Critical Hyperkalaemia
Question 2. (1 mark)
What is the anion gap?
Must include: 39 (no K+ included) or 29 (K+ included)
Question 3. (2 marks)
What management will you institute?
Must include:
- Cessation of resuscitation, as the patient is clearly dead
- Documentation of same and inform coroner and family
Question 4. (2 marks)
A member of your team objects to cessation of resuscitation on the basis of the patient’s temperature, suggesting that the patient should be actively rewarmed before she can be pronounced dead. How will you respond?
Must include thematically:
- This patient’s temperature is a product of her death, rather than the cause of her asystole (she is not “cold and dead”, but rather is “dead and cold”).
- There are multiple indications of futility (age, asytole, potassium, pH) and therefore resuscitation should be ceased.
saq 5.
A 28 year old female is brought to your emergency department after being run over by a motorbike. There is no suggestion of a head or chest injury, and she has tire marks on her abdomen. A pelvic binder is in situ, and there are no long bone fractures or external sites of compressible haemorrhage. The injury occurred 40 minutes prior to arrival in the ED.
Her vital signs are:
- HR 136 /min
- BP 85/68 mmHg
- RR 26 /min
- Sats 99% RA
- T 35.6 oC
A venous gas lactate on arrival is 4.6 mmol/L.
Question 1. (5 marks)
Give 5 interventions you will apply for the resuscitation of this patient.
Must include the elements of:
Management:
- Transfusion with warmed packed red cells
- Co-administration of FFP and plt in a 1:1:1 ratio
- Administration of cryoprecipitate after 6 units PRC
- Replacement of serum calcium to ensure normal ionized Ca++
- Administration of TXA 1g stat then 1g infused over 8 hours
Question 2. (5 marks)
Give 5 clinical or laboratory endpoints you will assess as markers of the efficacy of your resuscitation.
Endpoints
- SBP 90 mmHg
- HR approaching 100bpm
- Cap refill 2s
- Serum lactate <2.0
- Urine output >0.5ml/kg.hr
Question 3. (3 marks)
Briefly outline the evidence for the use of low blood pressure targets in trauma resuscitation.
Must include (thematically):
- one study of penetrating trauma patients
- showed a reduction in mortality with low rather than high volume BP targets
- there is no evidence for blunt trauma patients.
SAQ 6.
A 50 year old man is brought in by the ambulance after a VF cardiac arrest. The ambulance report 10 minutes of CPR at the scene followed by one successful 200J shock. The patient was unresponsive after this, so the intensive care paramedic present has performed an RSI with confirmed tube placement.
The patient's vital signs are:
HR 90
BP 95/66 mmHg
RR 16 (ventilated by BVM on 100% O2)
Sats 99%
T 37.3 oC
Question 1. (6 marks)
Give 3 initial investigations you will conduct in this patient and a rationale for each.
Must include:
- Blood sugar level: altered level of consciousness
- ECG: assess indication for urgent cardiac catheterisation
- urgent UEC/VBG: check K+ in context of VF in case urgent treatment is required.
Question 2.
Give 7 strategies you will apply to facilitate effective ventilation and neuroprotection in this patient.
Must include:
- ventilate at 30 degrees head up
- aim low normal CO2
- maintain normal PO2 at 100% sats/100mmHg
- decompress stomach with NGT
- sedate with appropriate agents (agent must be specified e.g. morphine/midazolam 1/1mg per ml)
- paralyse with an appropriate agent (e.g. vecuronium 10mg)
- cool with initial cold fluid bolus
Question 3. (4 marks)
Summarise the evidence for the use of therapeutic hypothermia in this patient.
Must include:
2 studies from 2002 examined cooling to 33oC in
- post VF out of hospital arrest versus maintenance of normal temperature
- there was improved neurologic outcome in the cooled patients compared to the non cooled patients
(for reference only the two studies are the HACA study and the Bernard Study)
However the Targeted Temperature Management study published in 2013 suggested:
- there was no difference in outcome between cooling to 33 and 36 degrees
- for all out of hospital cardiac arrest patients.
The patient's vital signs are:
HR 90
BP 95/66 mmHg
RR 16 (ventilated by BVM on 100% O2)
Sats 99%
T 37.3 oC
Question 1. (6 marks)
Give 3 initial investigations you will conduct in this patient and a rationale for each.
Must include:
- Blood sugar level: altered level of consciousness
- ECG: assess indication for urgent cardiac catheterisation
- urgent UEC/VBG: check K+ in context of VF in case urgent treatment is required.
Question 2.
Give 7 strategies you will apply to facilitate effective ventilation and neuroprotection in this patient.
Must include:
- ventilate at 30 degrees head up
- aim low normal CO2
- maintain normal PO2 at 100% sats/100mmHg
- decompress stomach with NGT
- sedate with appropriate agents (agent must be specified e.g. morphine/midazolam 1/1mg per ml)
- paralyse with an appropriate agent (e.g. vecuronium 10mg)
- cool with initial cold fluid bolus
Question 3. (4 marks)
Summarise the evidence for the use of therapeutic hypothermia in this patient.
Must include:
2 studies from 2002 examined cooling to 33oC in
- post VF out of hospital arrest versus maintenance of normal temperature
- there was improved neurologic outcome in the cooled patients compared to the non cooled patients
(for reference only the two studies are the HACA study and the Bernard Study)
However the Targeted Temperature Management study published in 2013 suggested:
- there was no difference in outcome between cooling to 33 and 36 degrees
- for all out of hospital cardiac arrest patients.
SAQ 7.
A 38 year old opiate overdose has been intubated by your registrar in the resus room for the purposes of airway protection. You have been called to see the patient as there is some difficulty with ventilation. The patient was intubated 15 minutes previously and the end tidal CO2 has continued to rise despite increasing the minute volume.
The patient’s vital signs are:
HR 118 /min
BP 120/83 mmHg
RR ventilated at 20/min x 500ml TV
Sats 100% 30% O2
T 40.1 oC
Your registrar reports that the patient was intubated with succinyl choline 150mg and ketamine 150mg.
An arterial blood gas is shown below.
pH 7.13
pO2 149 mmHg
pCO2 56 mmHg
HCO3- 16 mmol/L
Na+ 140 mmol/L
K+ 6.8 mmol/L
Cl- 104 mmol/L
Lactate 0.6 mmol/L
Question 1. (5 marks)
Describe two acid-base disturbances present in the gas above, calculate the expected compensatory response for each and comment on the results.
Must include:
- respiratory acidosis: expect HCO3- acutely for CO2 of 56 to be 21.5mmol/L
- metabolic acidosis: expect CO2 for HCO3- 16 = 32mmHg
Therefore no compensation is present and these are both primary disturbances.
Question 2. (4 marks)
Give 2 calculated values that support your appraisal of the metabolic arm of the disturbance and comment on each.
1. ANION GAP = 20 (no K+ included) This is High (RAGMA)
2. DELTA RATIO = 8/8 = 1.0. Confirms isolated RAGMA.
Question 3. (2 marks)
What is the most likely diagnosis?
Must include:
Malignant hyperthermia.
Question 4. (4 marks)
Give two pathology tests you will order to assess for complications of this condition, and the state the complication you are assessing for.
Must include:
CK – rhabdomyolisis
Coag/DIC screen - DIC
Question 5. (4 marks)
Give 4 management steps you will now undertake.
Suggested inclusions, mandatory in bold (pass criteria)
The patient’s vital signs are:
HR 118 /min
BP 120/83 mmHg
RR ventilated at 20/min x 500ml TV
Sats 100% 30% O2
T 40.1 oC
Your registrar reports that the patient was intubated with succinyl choline 150mg and ketamine 150mg.
An arterial blood gas is shown below.
pH 7.13
pO2 149 mmHg
pCO2 56 mmHg
HCO3- 16 mmol/L
Na+ 140 mmol/L
K+ 6.8 mmol/L
Cl- 104 mmol/L
Lactate 0.6 mmol/L
Question 1. (5 marks)
Describe two acid-base disturbances present in the gas above, calculate the expected compensatory response for each and comment on the results.
Must include:
- respiratory acidosis: expect HCO3- acutely for CO2 of 56 to be 21.5mmol/L
- metabolic acidosis: expect CO2 for HCO3- 16 = 32mmHg
Therefore no compensation is present and these are both primary disturbances.
Question 2. (4 marks)
Give 2 calculated values that support your appraisal of the metabolic arm of the disturbance and comment on each.
1. ANION GAP = 20 (no K+ included) This is High (RAGMA)
2. DELTA RATIO = 8/8 = 1.0. Confirms isolated RAGMA.
Question 3. (2 marks)
What is the most likely diagnosis?
Must include:
Malignant hyperthermia.
Question 4. (4 marks)
Give two pathology tests you will order to assess for complications of this condition, and the state the complication you are assessing for.
Must include:
CK – rhabdomyolisis
Coag/DIC screen - DIC
Question 5. (4 marks)
Give 4 management steps you will now undertake.
Suggested inclusions, mandatory in bold (pass criteria)
- Switch to IV sedation with a safe combination of agents (which must be specified eg morphine & midazolam 1/1mg per ml run at 5ml/hr)
- Discontinuation of suxamethonium
- Hyperventilation at 2-3x normal minute volume
- Administer dantrolene 2.5mg/kg IV repeated every 5 minutes until 10-20mg/kg has been administered or reaction ceases
- Actively cool the patient with ice packs at groin/axilla or warm IV fluids
SAQ 8. (Note follows into saQ 9 as a double question).
A 19 year old male is brought into your department by ambulance with severe cramps in his arms and legs. He is alert and oriented, and has been brought in from running a 20km race.
His vital signs are:
HR 110 /min
BP 88/66 mmHg
RR 33 /min
Sats 99% RA
T 40.1 oC
His venous gas on arrival is shown below.
pH 7.15
pCO2 30 mmHg
PO2 38 mmHg
HCO3- 15 mmol/L
BE -5
Na+ 140 mmol/L
K+ 7.1 mmol/L
Cl- 107 mmol/L
Urea 15.6 mmol/L
Creatinine 300 umol/L
Question 1. (6 marks)
Using the table below give 3 acid base disturbances that are present, and indicate if each is primary or compensatory.
His vital signs are:
HR 110 /min
BP 88/66 mmHg
RR 33 /min
Sats 99% RA
T 40.1 oC
His venous gas on arrival is shown below.
pH 7.15
pCO2 30 mmHg
PO2 38 mmHg
HCO3- 15 mmol/L
BE -5
Na+ 140 mmol/L
K+ 7.1 mmol/L
Cl- 107 mmol/L
Urea 15.6 mmol/L
Creatinine 300 umol/L
Question 1. (6 marks)
Using the table below give 3 acid base disturbances that are present, and indicate if each is primary or compensatory.
|
DISTURBANCE.
1. Raised anion gap metabolic acidosis 2. Non anion gap metabolic acidosis 3. Respiratory alkalosis |
PRIMARY/COMPENSATORY?
1. Primary 2. Primary 3. Compensatory. |
Question 2. (3 marks)
Provide 3 calculations to support your answer above.
1. Expected CO2 for HCO3 = 8 + 1.5 x 15 = 30.5 mmHg
2. ANION GAP = 18 HIGH
3. DELTA RATIO = 6/9 = 0.6. Suggests concommittant NAGMA.
Question 3. (3 marks)
Give 3 other major abnormalities present on the pathology.
Must include:
- life threatening hyperkalaemia
- grossly raised renal indices (urea and creatinine)
Question 4. (2 marks)
What is the likely cause of this patient’s illness? Provide a calculation to support your answer.
This patient likely has rhabdomyolysis from acute heat illness
The U:C ratio of 50% suggests intrinsic renal failure (possibly from myoglobin) rather than pre-renal failure due to dehydration.
Question 5. (1 mark)
What further investigation will you add on to this patient’s pathology to confirm your diagnosis?
Must include: CK
Provide 3 calculations to support your answer above.
1. Expected CO2 for HCO3 = 8 + 1.5 x 15 = 30.5 mmHg
2. ANION GAP = 18 HIGH
3. DELTA RATIO = 6/9 = 0.6. Suggests concommittant NAGMA.
Question 3. (3 marks)
Give 3 other major abnormalities present on the pathology.
Must include:
- life threatening hyperkalaemia
- grossly raised renal indices (urea and creatinine)
Question 4. (2 marks)
What is the likely cause of this patient’s illness? Provide a calculation to support your answer.
This patient likely has rhabdomyolysis from acute heat illness
The U:C ratio of 50% suggests intrinsic renal failure (possibly from myoglobin) rather than pre-renal failure due to dehydration.
Question 5. (1 mark)
What further investigation will you add on to this patient’s pathology to confirm your diagnosis?
Must include: CK
SAQ 9
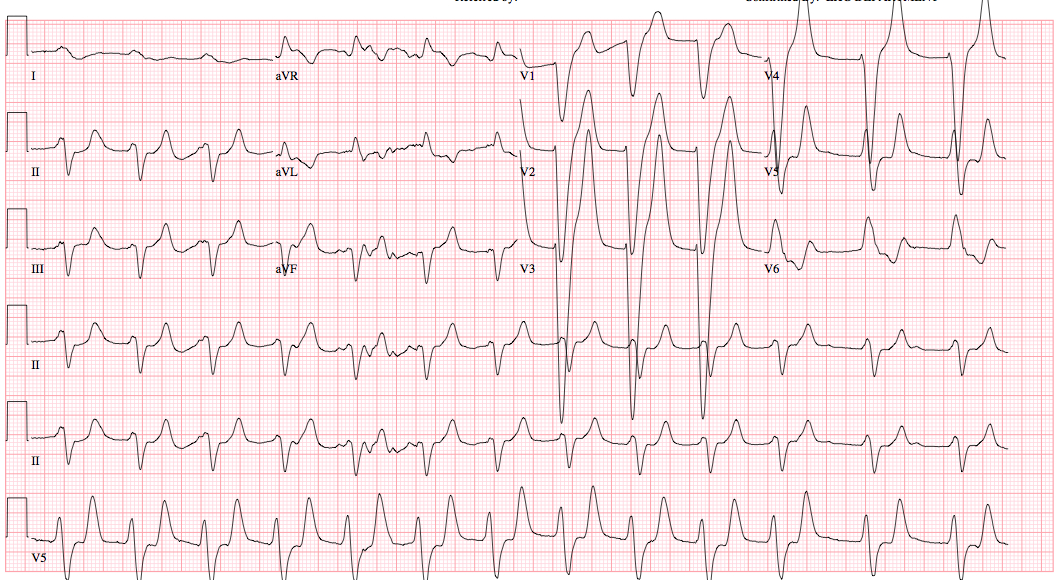
The patient from SAQ 8 has an ECG, which is shown below.
Question 1.
Give 4 abnormalities seen on the ECG (4 marks)
Must include:
Wide QRS
Short PR
Tented T waves
Northwest axis
Question 2. (4 marks)
Give 4 treatments you will specifically give in response to this ECG.
Treatments
Question 3. (6 marks)
The patient’s CK titre returns at 15 000 IU/L. Using the table below list 3 therapeutic issues in this patient, and outline how you will treat each one.
Give 4 abnormalities seen on the ECG (4 marks)
Must include:
Wide QRS
Short PR
Tented T waves
Northwest axis
Question 2. (4 marks)
Give 4 treatments you will specifically give in response to this ECG.
Treatments
- Administration of calcium gluconate or calcium carbonate
- Sodium bicarbonate 50ml 8.4%
- Insulin 10U plus dextrose 25-50ml 50%
- Neb salbutamol 5mg
Question 3. (6 marks)
The patient’s CK titre returns at 15 000 IU/L. Using the table below list 3 therapeutic issues in this patient, and outline how you will treat each one.
|
ISSUES
1. Hyperthermia 2. Renal failure from rhabdomyolysis 3. Symptomatology (aches/cramps) |
TREATMENT
1. Cooling: ice packs/cold fluids 2. Fluid at high rates 150ml/hr plus aimed to urine output >1mg/kg 3. Pain relief: paracetamol 1g PO |
Question 4. (4 marks)
List 4 methods you will use to begin cooling this patient.
Must include any of:
Removal of clothes
Spraying with tepid water and fanning
Ice packs in groing and axillae
Administration of cooled fluids intravenously
Use of a cooling blanket or other apparatus
List 4 methods you will use to begin cooling this patient.
Must include any of:
Removal of clothes
Spraying with tepid water and fanning
Ice packs in groing and axillae
Administration of cooled fluids intravenously
Use of a cooling blanket or other apparatus
saq 10.
Using the table below compare and contrast neuroleptic malignant syndrome and malignant hyperthermia.
|
FEATURE
Causative agent and an example (4 marks) Onset (2 marks) Clinical features (3 each for 6 marks total) Treatment principles (4 marks) |
NMS
Neuroleptic agents (e.g. phenothiazines) Idiosyncratic (most common after 4-14 days, but can present any time) Fever Rigidity Altered mental status Removal of antiopsychotic agent Supportive care |
Malignant Hyperthermia
Depolarizing muscle relaxants (suxamethonium) and inhalation anaesthetics (e.g. sevoflurane) Onset minutes after exposure Any of: Fever Rising end tidal CO2 Muscle rigidity Tachycardia Rhabdomyolysis Cease anaesthetic Dantrolene 2.5mg/kg up to 10.5 mg/kg |