|
Stuff you’ll never see….but just in case. Occasionally the examination throws up stuff we just don’t expect will be present. Part of preparation is both casting a wide net so that it’s unlikely you’ve missed anything important, and also understanding that there is logic and rules to how the examination is played. Take the following question: You are called to attend a 38yo P1G0 woman who is 38/40. She has presented to your department with severe rhythmic cramping in the abdomen. A midwife has attended from birth suite and hands you a CTG which is shown below. Describe and interpret the CTG and outline your actions. 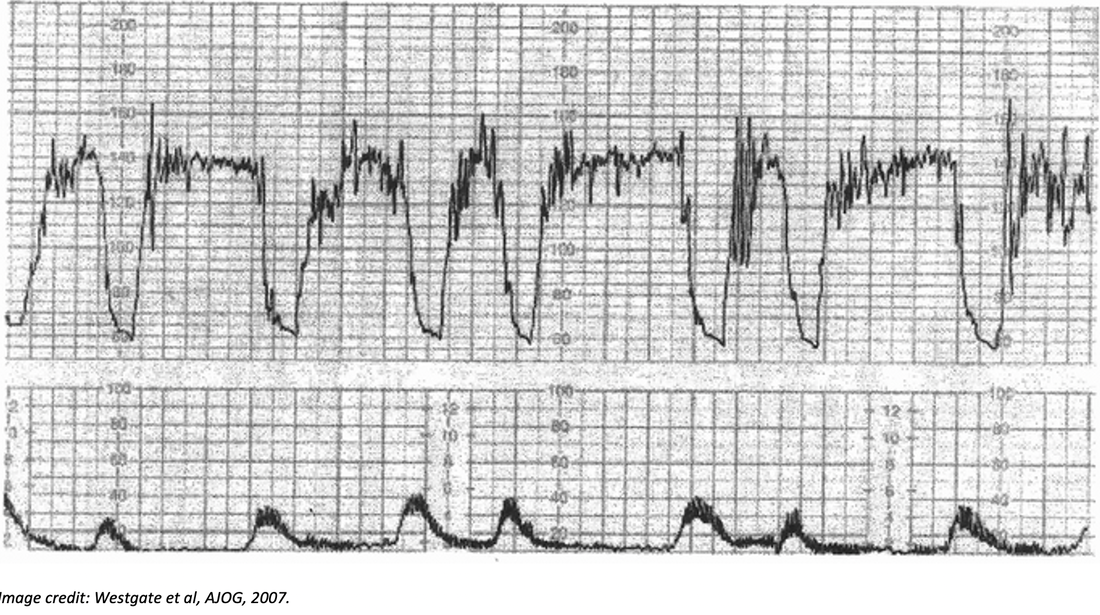 So, before you think “this is completely ridiculous and would never happen in real or exam life”, there was a CTG question on a recent exam.
Step back for a moment, and ask yourself what you’d do with this. Next week, we’ll get a brief outline of CTGs into the FPFF. But, if you’ve never seen this before, take a moment and have a think about how you might answer. Can you use exam smarts….? Here’s an example of what that might look like. i.“This is the emergency medicine exam. It’s highly likely that the prop I have been given shows a significant emergency. a.It might be a normal prop, but this is far less likely ii.This is not a test routinely reviewed by Emergency Physicians. a.I won’t be expected to have detailed in depth knowledge of subtleties b.In other words, the findings should be pretty obvious. iii.CTGs are done for ? foetal distress. It is therefore highly likely that this is what is shown on the CTG. iv.Therefore, even knowing nothing about CTGs, with the context of a woman in advanced pregnancy in abdominal pain, I would guess and say that the CTG is most likely to show significant signs of foetal distress. v.I know that CTGs measure foetal Heart Rate. vi.Therefore I will answer with the elements of the CTG shows foetal bradycardia and urgent obstetric intervention is needed to deliver the baby. a.I might not get all the marks, but hopefully I’ll get enough to pass. b.If I’m wrong, there are no negative marks, so what do I have to lose.” You might think that’s pretty out there. It is. And it’s certainly not a way to practice medicine in real life. But, in preparing for the examination, we are believers in using every strategy available when the occasion calls for it. If knowledge and experience fail, try stepping back and thinking about *why* you are being asked the question, rather than just the content of the question itself.
0 Comments
Leave a Reply. |
AuthorShareThe Written Fellowship Course has its beginnings back in 2007, When Dr Kas started it at RPA in Sydney. It was then called the Kamikaze Course. Archives
March 2021
Categories |
 RSS Feed
RSS Feed