|
This week at fellowshipexam.com we are taking on two of the most feared props in the exam itself – the ECG and the ABG. In particular, the ABG seems to be a source of significant concern for most candidates. The bad news is that even with the advent of the new examination the ABG plays a starring role. In the 2015.1 exam 2 of the thirty questions features were centred on an ABG. That’s just about 7 % of the marks available for a single prop. "The good news is that with a systematic approach the ABG can be broken down easily..." The good news is that with a systematic approach the ABG can be broken down easily and those marks collected. Let’s look at question 23, which features a HARD blood gas…. 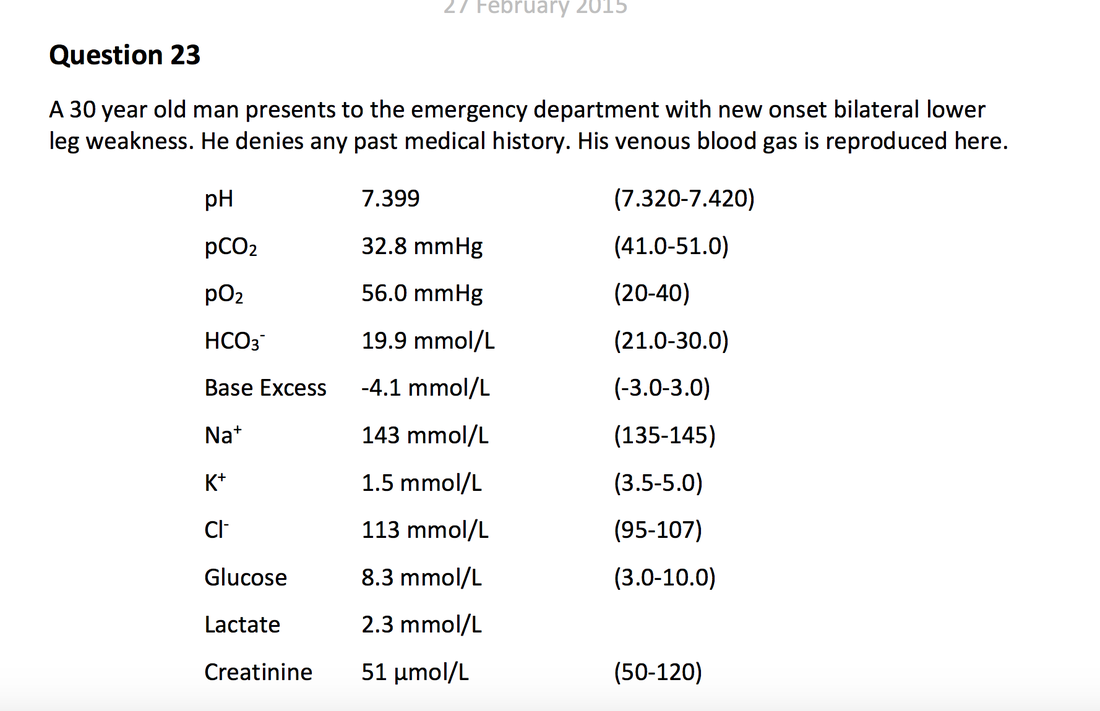 After being presented with this monstrosity we are asked four questions.
All in six minutes! We reiterate our opinion that this question is hard! Right, so a systematic approach to the ABG is necessary. We teach the Own the ABG approach. Looking at the Acid-Base balance we can note immediately:
So, working through the ABG systematically we can answer the questions pretty easily. Our answers and comments are below.
Although some of the questions in this examination stunner are a bit opaque for us, we remain convinced that a systematic approach to props like the ABG puts candidates in the best position to succeed. We've set our course candidates a number of ABGs to practice, and we're planning on discussing the issue in more depth at our FACE-TO-FACE meeting in Melbourne. As always we'll be preaching that a systematic approach and practice are what yield the best chance for success on the big day.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
TAKE ME TO THE COURSE PORTAL!
The fellowship facultyWe work as emergency physicians, and teach, blog and write at resus.com.au Archives
July 2017
Categories |
 RSS Feed
RSS Feed